GALEAZZI FRACTURE-DISLOCATION
• Definedas a fracture of the radial diaphysis
(typically distal 1/3) with a dislocation of the
DRUJ
• First described in 1822 by Sir Astley Cooper
• Further described by Galeazzi in 1934
• Frequently underdiagnosed
• Most likely to occur within 7.5cm of
midarticular surface of distal radius (Rettig and
Raskin)
7.
MECHANISM
• Forceful axialloading of the forearm
with wrist extended and maximally
pronated
• Some authors believe loading in
supination can also result in the
injury
• Falls, MVC, electric shock, blunt
trauma
8.
ANATOMY: OSSEOUS
• Majorradial bow: from the biceps
tuberosity to the ulnar aspect of the
articular surface
– Essential for proper forearm
rotation
9.
ANATOMY: SOFT TISSUE
•Interosseous membrane
– Complex ligamentous structure that
firmly attaches the radius and ulna
– Transfers load from radius to ulna
– Terminates proximal to the distal 1/3
radial diaphysis
• Higher risk of shortening
10.
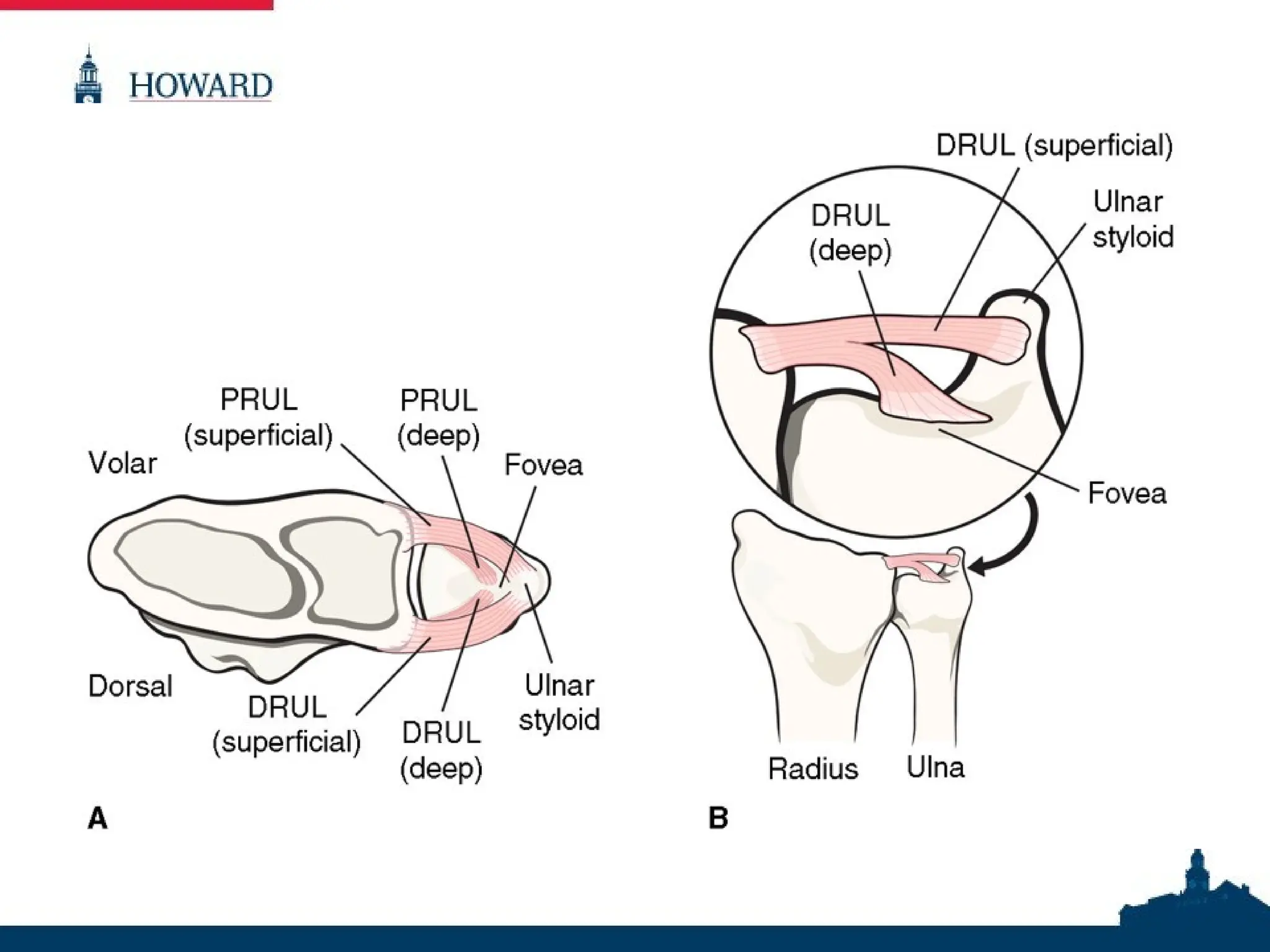
ANATOMY: SOFT TISSUE
•Triangular Fibrocartilage Complex (TFCC)
– Primary stabilizer of the DRUJ
– Base attaches to the junction of the
lunate fossa and the sigmoid notch
– Apex attaches to the fovea and ulnar
styloid
– Primary stabilizers of distal ulna: dorsal
and palmar radioulnar ligaments
12.
PATHOPHYSIOLOGY
• Radius fractures2/2 axial load
• The radius shortens, significant force is
pulled through the distal ulna via the TFCC
• The TFCC fails in its substance or through
avulsion of the ulnar styloid
• Without this ligamentous constraint, the
DRUJ is destabilized and the distal ulna
dislocates
IMAGING
• Radiographs ofthe elbow, wrist, and forearm
– AP
– True lateral
• Findings suggestive of DRUJ instability:
– Ulnar styloid fracture
– DRUJ widening (AP)
– Dislocation/subluxation of ulna relative to
radius (lateral)
– Radial shortening >5mm
15.
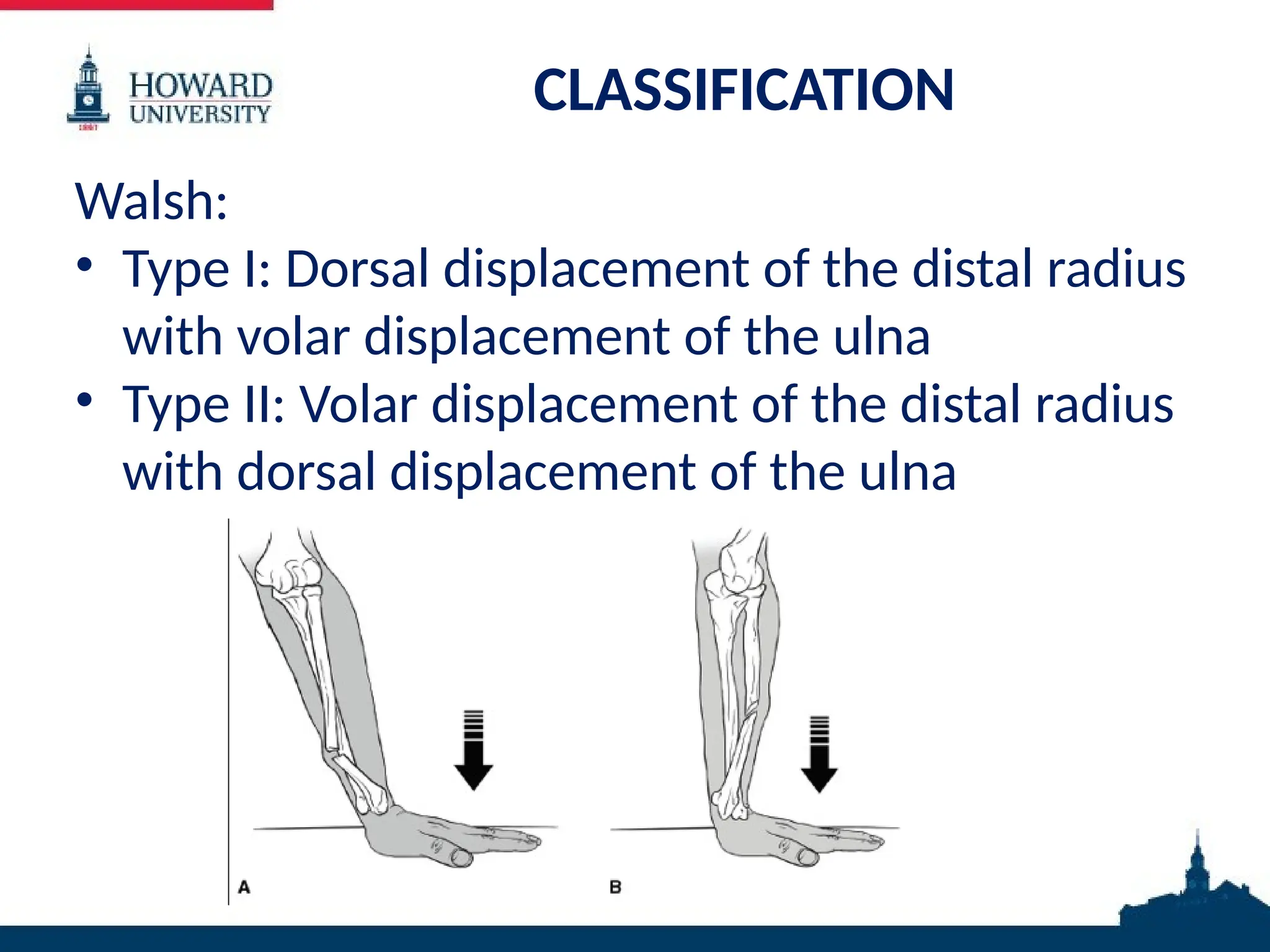
CLASSIFICATION
Walsh:
• Type I:Dorsal displacement of the distal radius
with volar displacement of the ulna
• Type II: Volar displacement of the distal radius
with dorsal displacement of the ulna
• an
ASSESSMENT
59 YO femalewith right distal 1/3 radial
diaphyseal fracture with associated DRUJ
dislocation
– Walsh type II
– Rettig and Raskin type I
– AO/OTA 22A2.3
19.
MANAGEMENT
Nonoperative
• Not indicated
•Fracture of necessity
• Historically, nonoperative treatment with closed
reduction and casting yielded poor outcomes
Operative
• ORIF radius
– Plate osteosynthesis
– Rush rod
– Percutaneous K-wire fixation
• +/- ORIF ulnar styloid, open reduction of DRUJ, closed
reduction and pinning of DRUJ
SUMMARY
• Largest studyof compression plating at that
time (n=55)
• Both dorsal and volar techniques used
– Superior results with dorsal, although volar
technically easier (mechanical limitation to
pronation)
• Functional outcomes excellent/good in 97% of
patients
• Radiographic healing in 97% patients
MATERIALS AND METHODS
•Purpose: to determine if fracture location has
an effect on DRUJ stability
• Retrospective
• 95 patients with Galeazzi fx
• Mean f/u: 6.8 months
24.
RESULTS AND CONCLUSION
•Results:
– 40/90 pts had residual DRUJ instability after
rigid fixation of radius
• 37 w/in 10cm of radial styloid
• 2 10-15cm
• 1 >15cm
• Conclusion:
– Proximity to radial styloid is predictive of DRUJ instability
requiring fixation after rigid radius fixation
MATERIALS AND METHODS
•Retrospective cohort study
• 66 patients
• Galeazzi fracture diagnosed intraoperatively
via DRUJ instability testing
27.
RESULTS AND CONCLUSION
•39% of fractures with residual DRUJ instability
located w/in 7.5cm of wrist joint (Rettig and
Raskin type I)
• 31% with shortening >5mm
• Conclusion: Radiographic guidelines for prediction of
Galeazzi lesion are only moderately accurate.
Intraoperative evaluation of the DRUJ should remain
the gold-standard
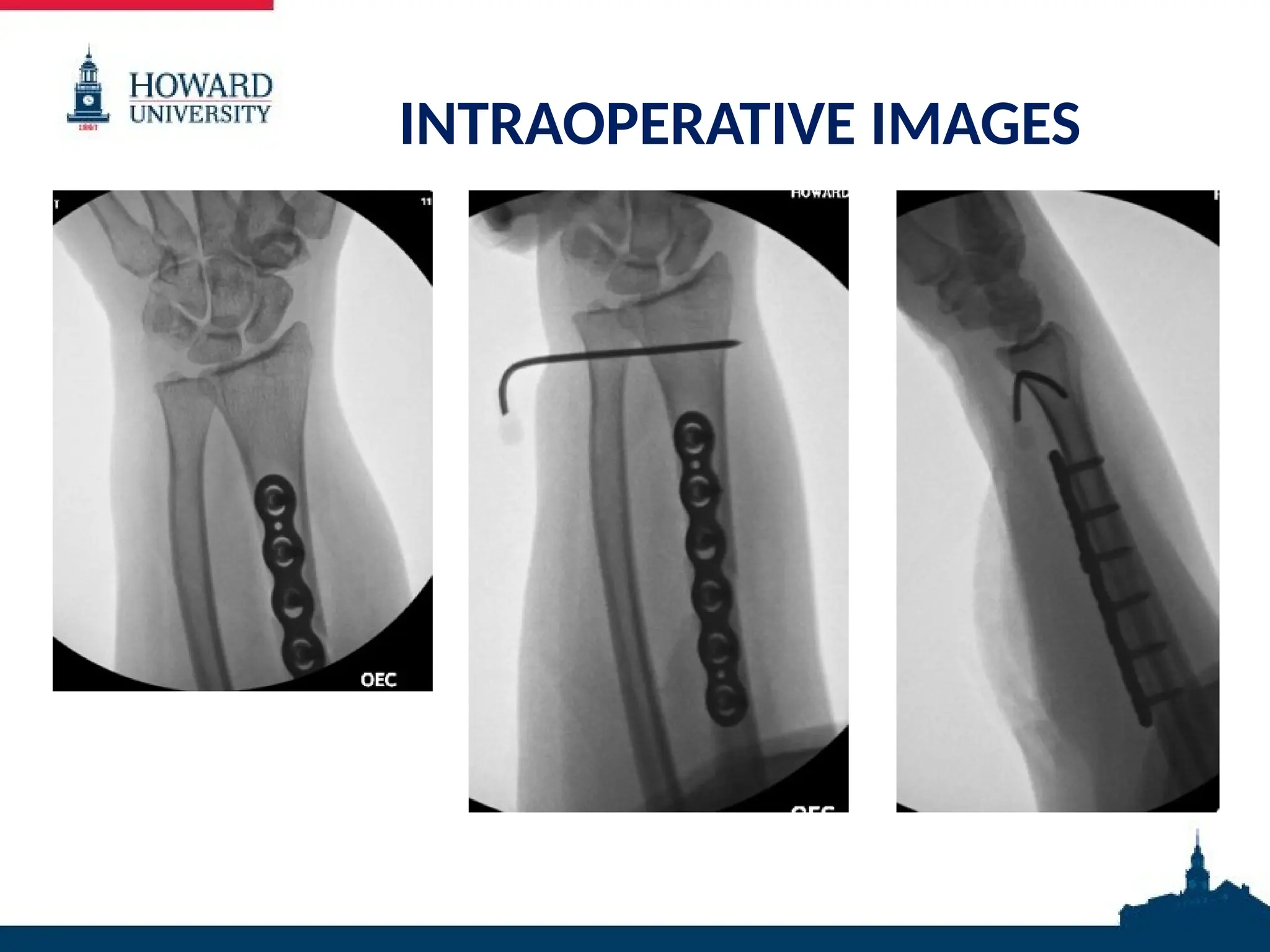
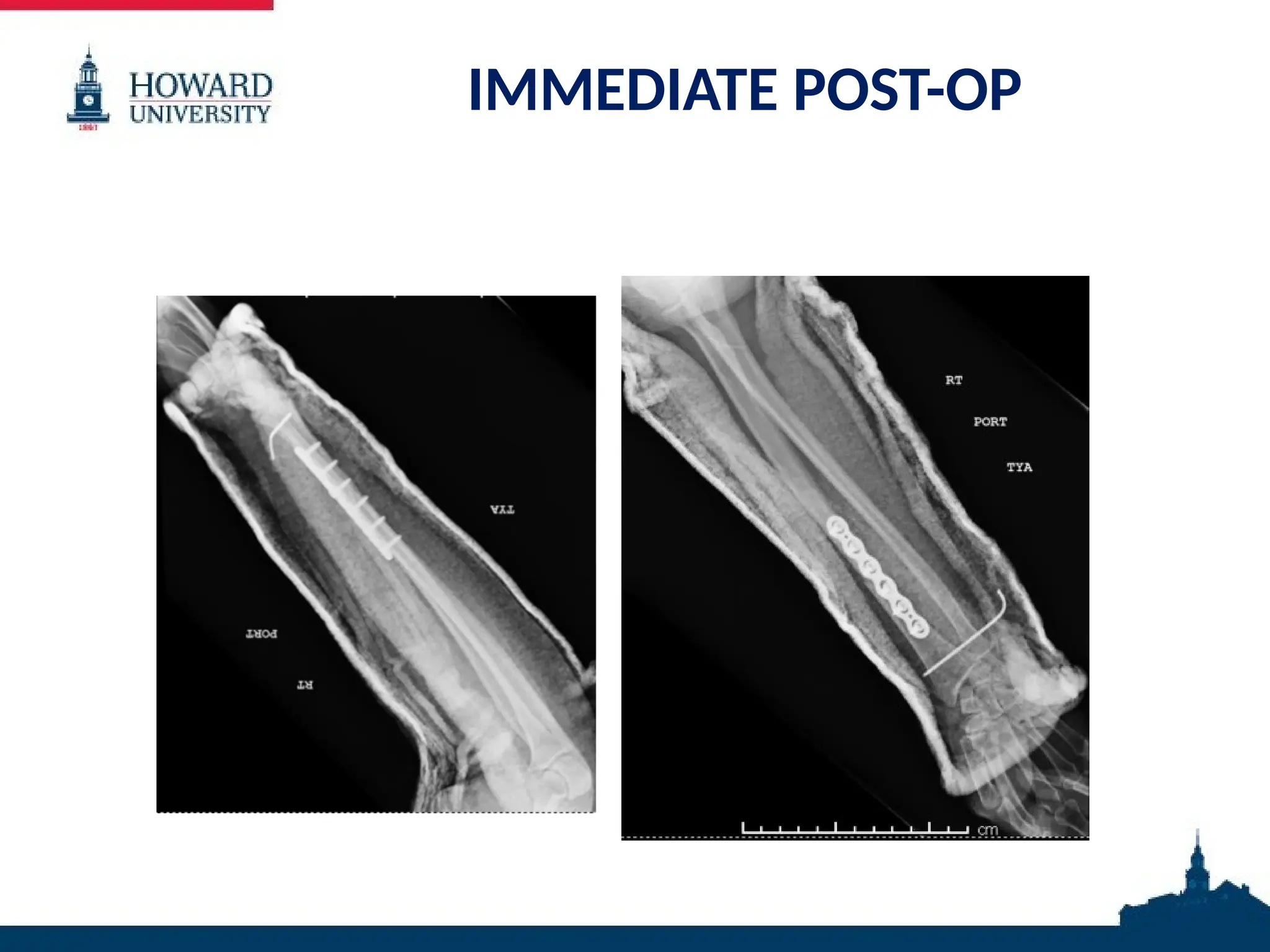
OPERATION IN BRIEF
•Volar approach of Henry
• Fracture reduced via longitudinal traction
• Reduction held with K-wire
• Dynamic compression plate applied
• Reduction judged anatomic
• DRUJ was found to be reduced after reduction
of radius
• Instability noted with both pronation and
supination, so K-wired placed across the DRUJ
#30 Posterior mal: provisionally fixed with a k wire. 1/3 tubular plate applied in buttress mode
Proximal long oblique posterior diaphyseal fx: also buttressed with 1/3 tubular plate after anatomic reduction
Plan was for addition fixation with distal tibial locking plate, but plate was dropped on the floor
Medial incision: articular surface visualized and anatomically reduced and provisionally fixed with k wires. Medial distal tibia locking plate
Syndesmosis was evaluated and judged to be stable
Closed primarily. Tension on medial incision, so wound vac applied
Splint, NWB



























![FOREARM_FRACTURES[1].pptx and management](https://cdn.slidesharecdn.com/ss_thumbnails/forearmfractures1-250813120934-75e3f6d7-thumbnail.jpg?width=640&height=640&fit=bounds)
























