Downloaded 60 times
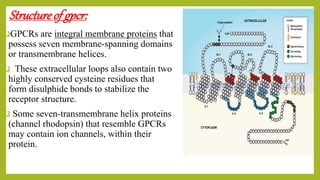

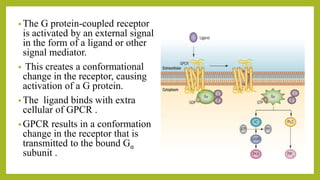
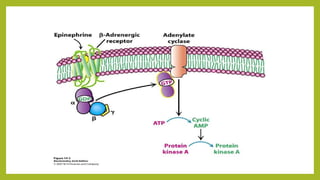



G-protein coupled receptors (GPCRs) are the largest family of membrane receptors found in humans. They have seven transmembrane domains and are activated by extracellular ligands binding, which causes a conformational change and activation of an intracellular G protein. This leads to second messenger signaling pathways involving cAMP or phosphatidylinositol. GPCRs regulate many physiological processes and are involved in behaviors, moods, and cellular responses. Their activity is modulated by phosphorylation, arrestins, and degradation of second messengers.




















































































