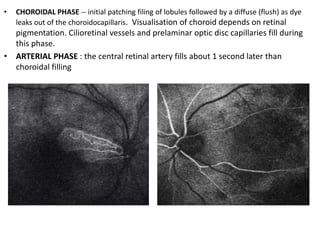
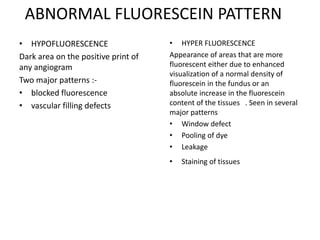
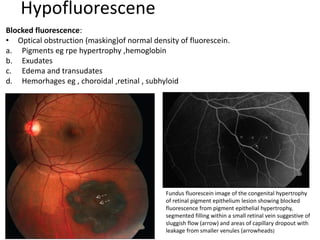
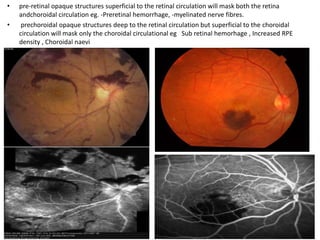
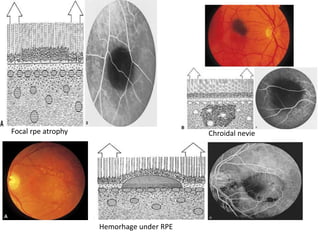
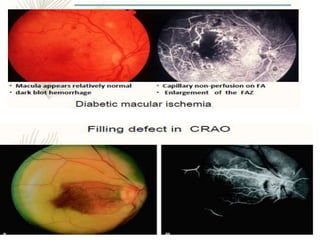
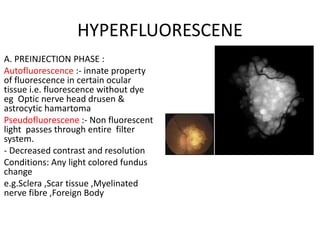
Fundus fluorescein angiography provides 3 key pieces of information: 1) the flow characteristics of blood vessels as fluorescein dye circulates through the retina and choroid, 2) fine details of the retinal pigment epithelium and retinal circulation, and 3) a clear picture of retinal vessels and assessment of their functional integrity. It involves injecting a fluorescent dye and taking rapid photographs under blue light to visualize the retinal and choroidal vasculature. Abnormal patterns include hypofluorescence from blocked fluorescence or vascular defects, and hyperfluorescence from window defects, leakage, pooling, or staining. It is useful for evaluating retinal diseases like epiretinal membranes, myopia, and diabetic retinopathy.


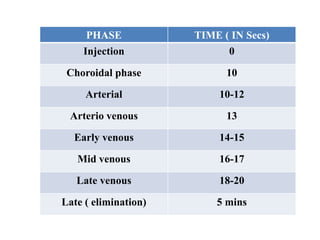
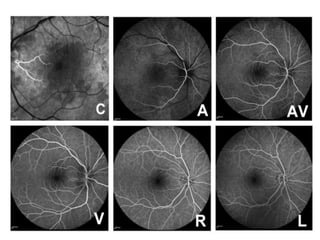
![1. PREARTERIAL [ CHOROIDAL FLUSH ] – 10 sec
2. ARTERIAL – 12sec
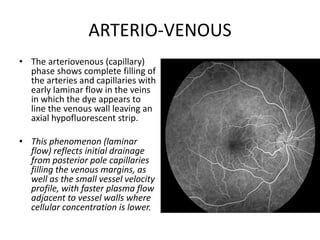
3. ARTERIO-VENOUS [ CAPILLARY ]
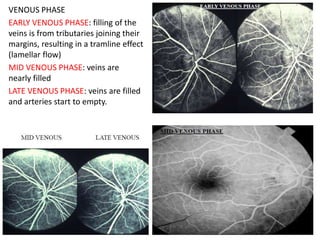
4. VENOUS – 30sec
-EARLY VENOUS
- MID VENOUS
- LATE VENOUS
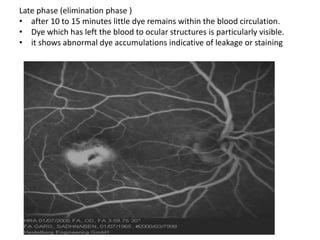
5. LATE ( ELIMINATION ) – after 10 min
PHASES OF ANGIOGRAM](https://image.slidesharecdn.com/fundusfl-200515084904/85/Fundus-fl-angio-15-320.jpg)