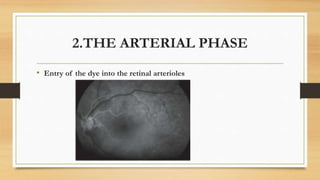
Fundus fluorescein angiography involves injecting a dye called sodium fluorescein intravenously and then photographing the retina as the dye circulates through the blood vessels. This allows visualization of the retinal and choroidal vasculature and detection of any abnormalities. The dye is absorbed by tissues and emits light at a higher wavelength when exposed to blue light, appearing green in the photographs. Areas of hypofluorescence or hyperfluorescence can indicate conditions like neovascularization or leakage. The angiogram proceeds through choroidal, arterial, venous, and late phases as the dye enters and clears from the blood vessels. While it provides valuable diagnostic information, limitations include inability to image the choroid directly and requirement for specialized