Downloaded 81 times
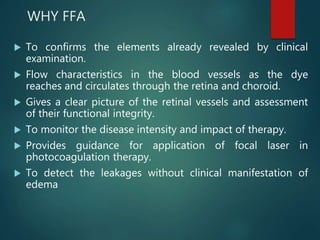

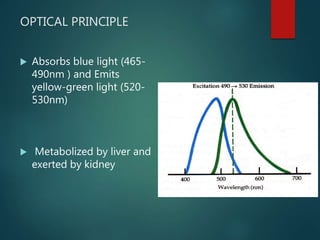

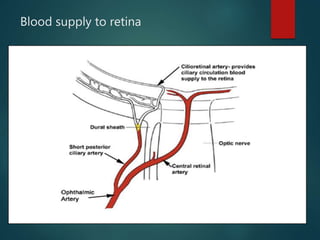
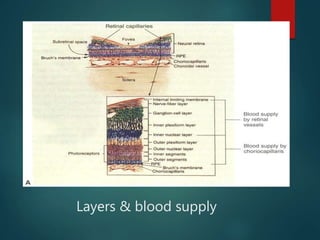
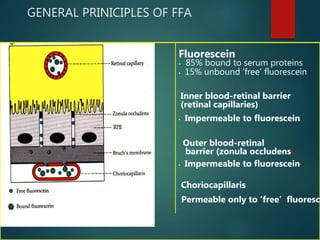
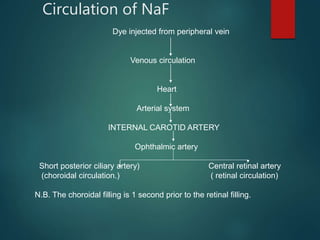
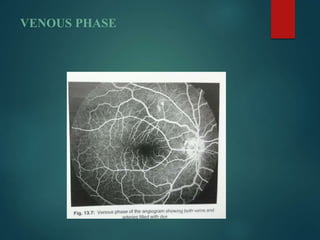
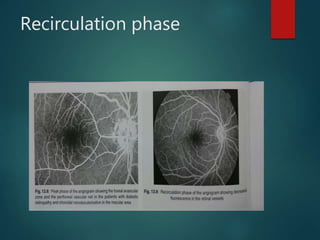
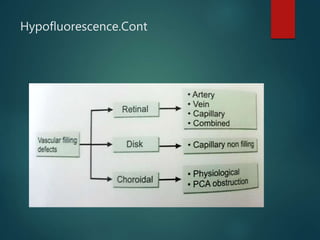
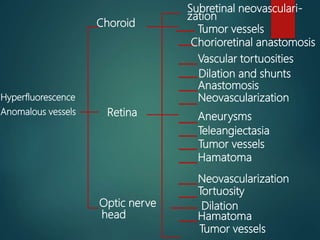
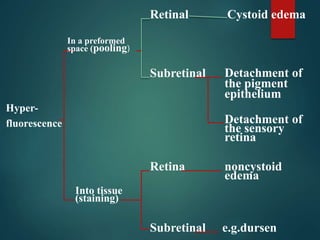
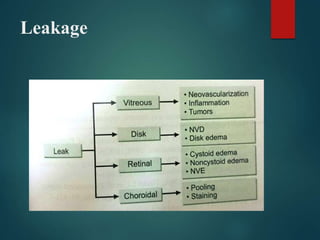
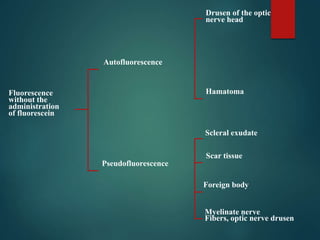
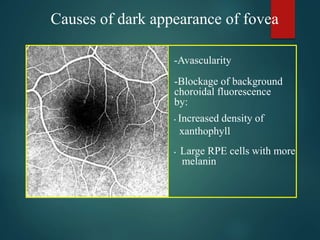
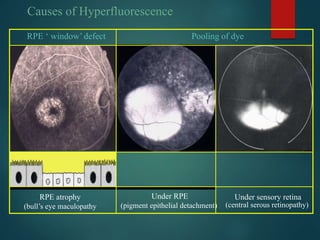

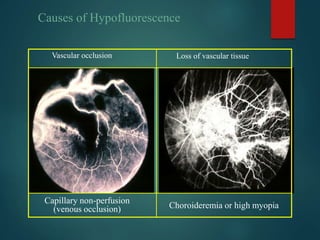
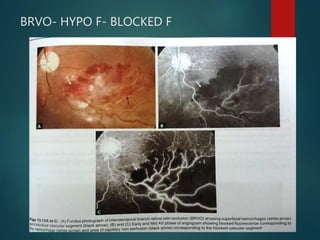
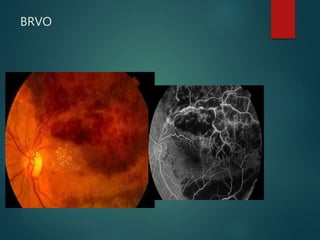
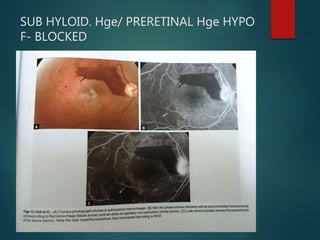
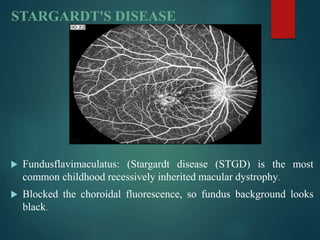
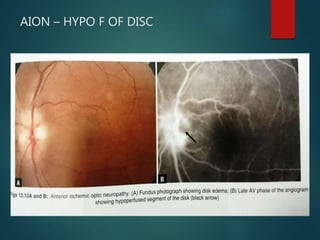
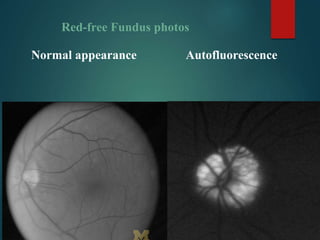
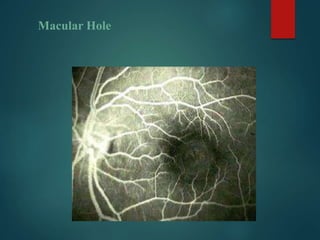
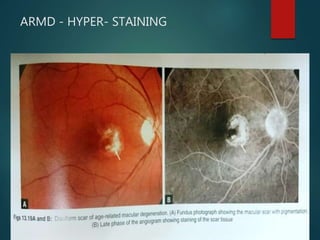

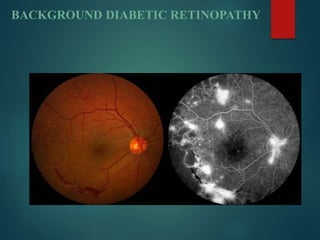
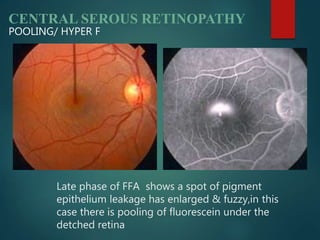
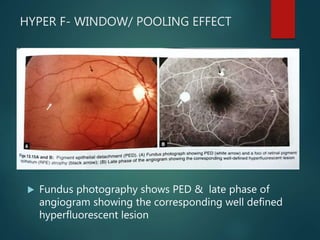
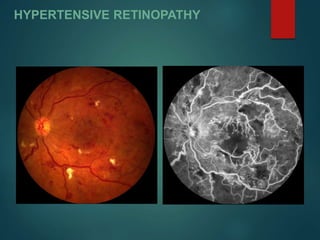

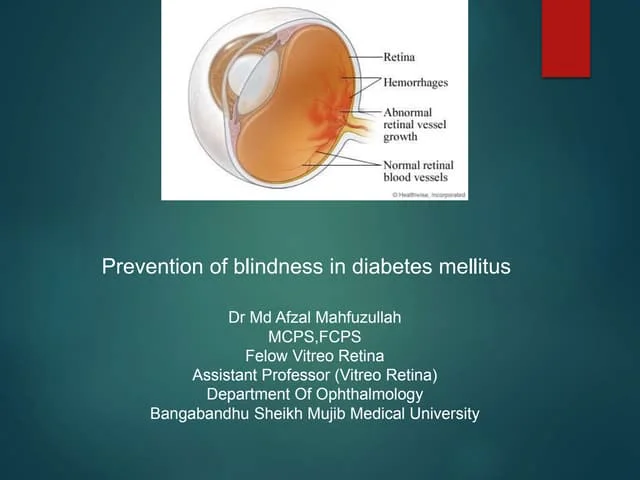
Fundus Fluorescein Angiography (FFA) provides detailed information about the retinal and choroidal circulation. It reveals inflammatory changes, lesions, neovascularization, fluid accumulation, and other abnormalities not visible on standard examination. FFA uses sodium fluorescein dye and filters to produce images of the retinal vasculature and detect leakage or blockages. Areas of hyperfluorescence indicate leakage or pooling of dye, while hypofluorescence shows blocked fluorescence from materials obstructing the view. FFA is useful for diagnosing and monitoring many retinal diseases.