Downloaded 14 times
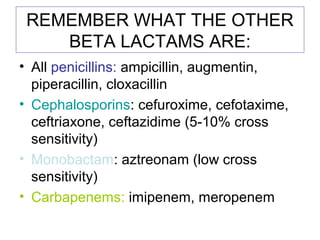
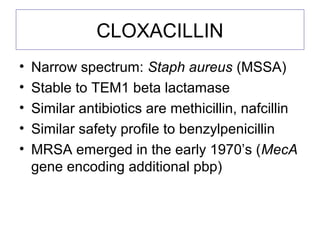
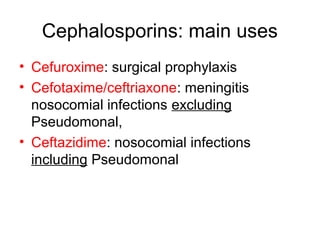
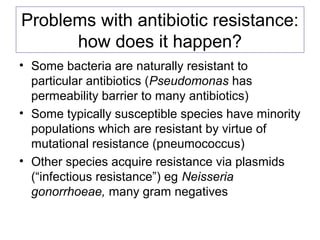

This document discusses several key principles of antibiotics: they are designed to selectively target bacteria while limiting toxicity to human cells. It provides examples of different antibiotic classes and their mechanisms of action, such as penicillin targeting the bacterial cell wall. Ideal antibiotics have narrow spectra, are bactericidal, and have few side effects. The document also covers antibiotic resistance development and challenges posed by resistant infections.



















































































