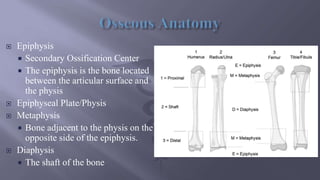
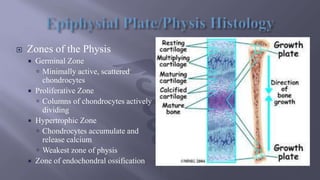
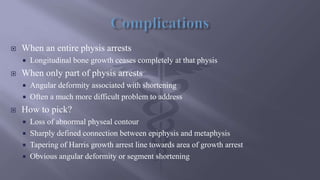
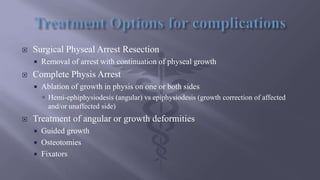
This presentation discusses epiphyseal injuries, also known as Salter-Harris fractures, which occur through the growth plate in children. It covers the anatomy of the growth plate and bone, the classification system for these fractures, which is important for determining treatment and prognosis. The most common classification is the Salter-Harris system, which is based on the fracture mechanism and its relationship to the physis. Treatment principles are to heal the fracture while maintaining growth potential. Management depends on the fracture type and may involve casting, closed reduction, percutaneous fixation, or open reduction and internal fixation. Complications like physeal arrest and deformity can occur and require further treatment.



































































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)

