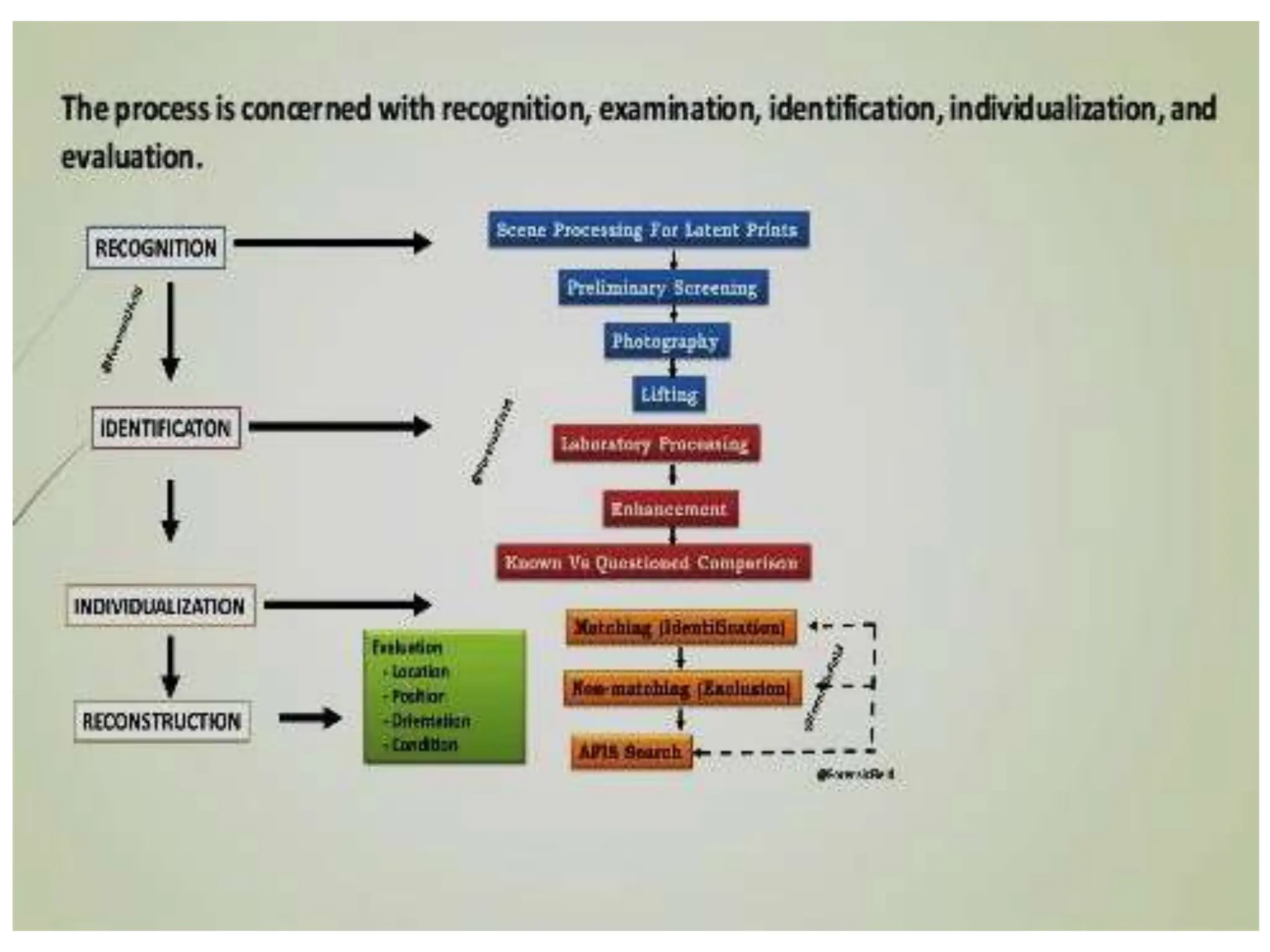
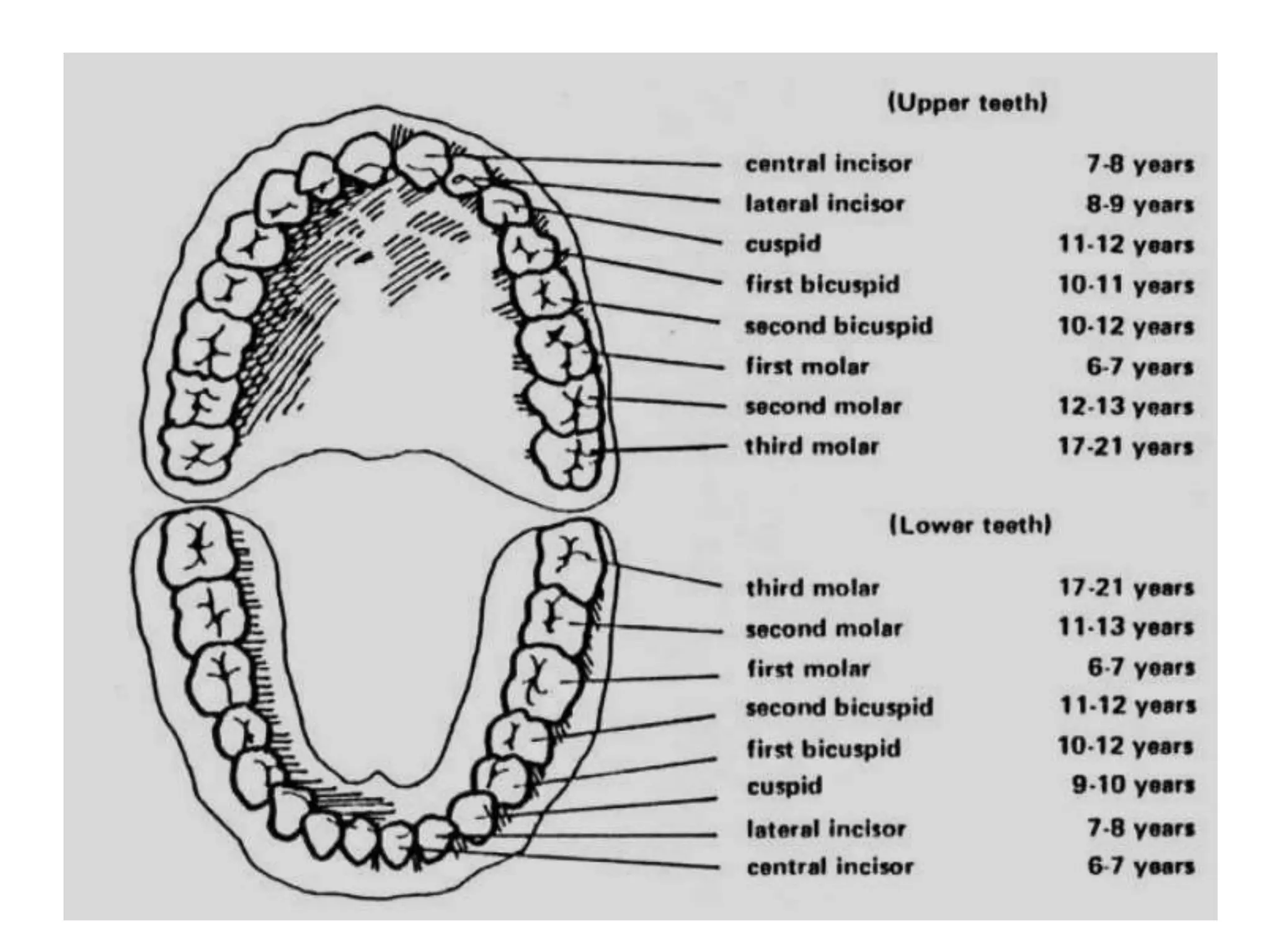
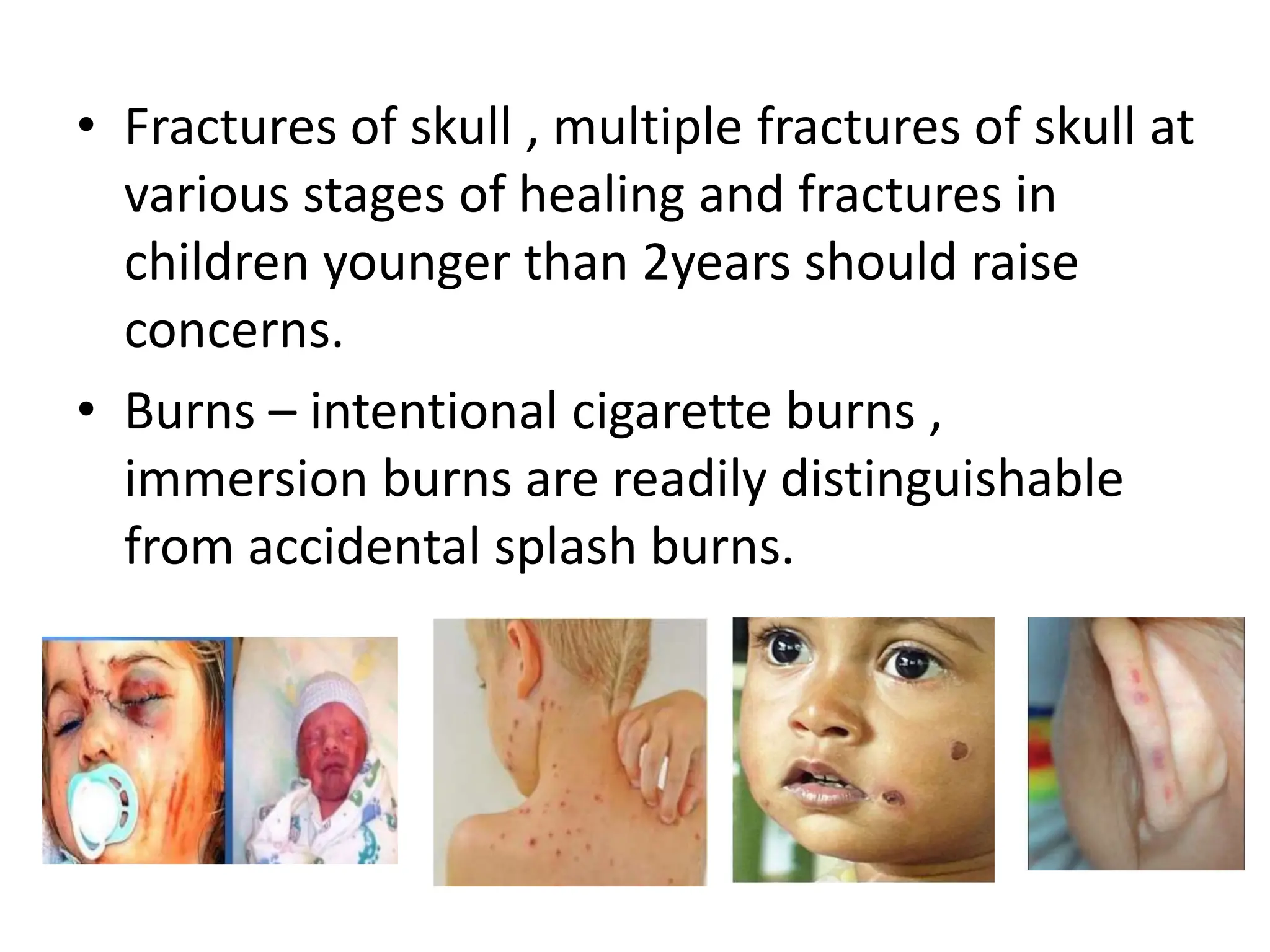
This document provides an overview of forensic odontology, which is the application of dental science to legal investigations. Some key areas discussed include dental identification procedures for human remains, analysis of bite marks, lip prints, and age estimation. Methods such as comparing dental records, DNA analysis from teeth, and examining characteristics like tooth size and morphology can be used to identify individuals. Forensic odontologists may also evaluate cases of child abuse and testify as expert witnesses in legal cases. The document outlines various techniques and how dental evidence can help solve crimes and identify victims.