
Downloaded 243 times
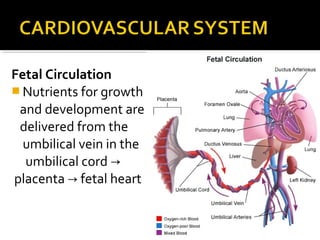
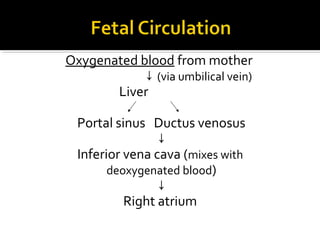
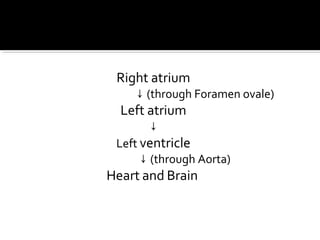
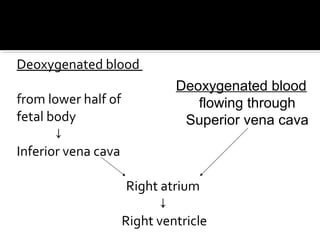
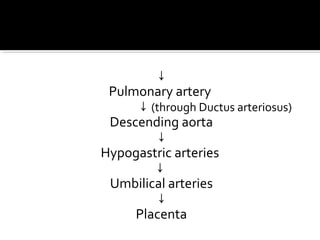
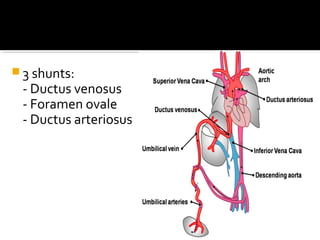
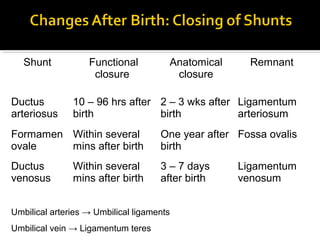

The document summarizes fetal circulation and development. Key points: 1. Fetal circulation involves three shunts that allow oxygenated blood to bypass the lungs and flow directly to the left side of the heart and brain. 2. After birth, the shunts close off and the circulation transitions to the adult pattern with blood flowing through the lungs. 3. Fetal organs develop throughout gestation, with the liver and bone marrow taking over hematopoiesis and the pancreas responding to changes in blood sugar with insulin production.

























































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)
















