Download as PDF, PPTX


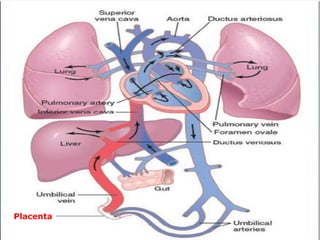

This document discusses the physiology of transition from fetal to newborn life. It outlines the major changes that occur at birth including the establishment of air breathing and changes in cardiovascular pressures and flows. The fetal circulation operates in parallel while the newborn circulation switches to series. At birth, the umbilical vessels and ducts close, the lungs aerate, and respiratory and cardiac functions are established. Abnormalities in the transition process can occur with preterm birth or C-section and may require assistance.



























































![CASE_PRESENTATION_ON_subdural_hematoma(SDH)[1 FINAL PPT]-1.pptx](https://cdn.slidesharecdn.com/ss_thumbnails/casepresentationonsubduralhematomasdh1finalppt-1-260129172522-d405d375-thumbnail.jpg?width=640&height=640&fit=bounds)


















