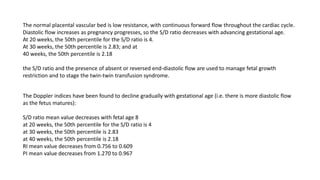
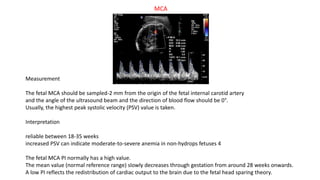
This document discusses fetal circulation and fetal echocardiography. It describes the normal Doppler waveform patterns seen in the umbilical artery, umbilical vein, ductus venosus and middle cerebral artery. It provides gestational age-based reference values for Doppler indices in the umbilical artery. The use of the cerebroplacental ratio as a marker of fetal wellbeing is also described. Measurement techniques and interpretation of Doppler studies of the middle cerebral artery and cerebroplacental ratio are covered.


















![Umbilical artery doppler [1]](https://cdn.slidesharecdn.com/ss_thumbnails/umbilicalarterydoppler1-210517112207-thumbnail.jpg?width=640&height=640&fit=bounds)












































































