Downloaded 128 times

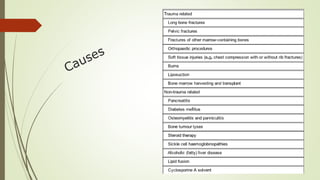
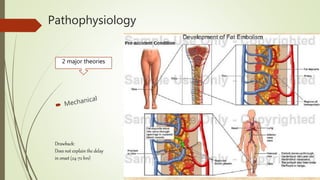
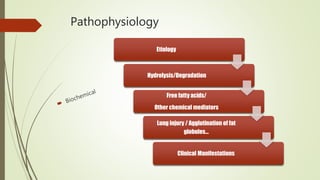

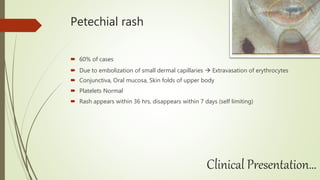


Fat embolism occurs when fat globules enter the bloodstream and become lodged in small blood vessels, potentially causing respiratory distress, neurological abnormalities, and a rash. It typically develops 1-3 days following long bone fractures or other trauma. The document discusses the pathophysiology, clinical presentation including respiratory changes, neurological features and petechial rash, diagnosis criteria, and management approaches such as immobilization, ventilation, fluid resuscitation, and in some cases prophylactic corticosteroids or ethanol administration.























































































