Download to read offline

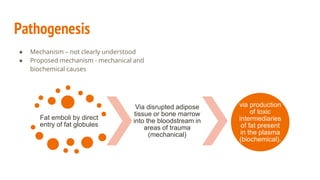


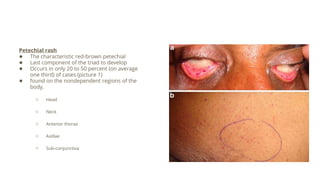
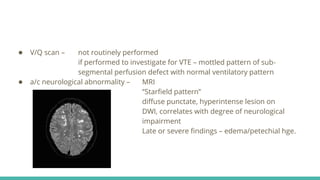
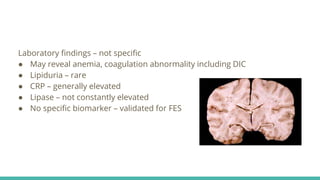
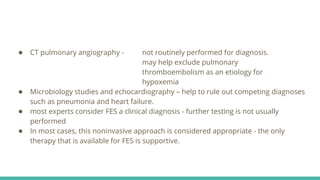


Fat embolism syndrome is a rare clinical syndrome caused by the presence of fat globules in the pulmonary circulation following trauma or other insults that release fat into the bloodstream. It is characterized by a clinical triad of hypoxemia, neurological abnormalities, and petechial rash that typically develops 24-72 hours after the initial injury. Diagnosis is clinical based on criteria sets, and treatment is supportive to address respiratory failure, shock, or other complications until it resolves spontaneously in days. Prevention focuses on early immobilization of fractures to reduce fat release and potential prophylactic corticosteroids, though their benefit is controversial.




























































![PERI-PROSTHETIC FRACTURE NAIL-PLATE CONSTRUCT [NPC].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/drarunkumardrmohamedashrafperiprostheticfrasturenail-plateconstructnpc-260209164459-7e9d15a1-thumbnail.jpg?width=640&height=640&fit=bounds)





![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)
