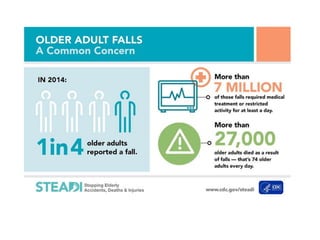
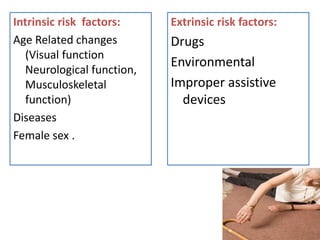
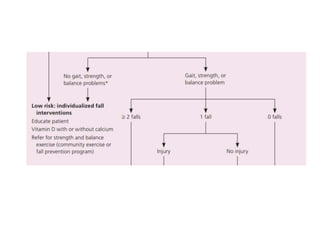
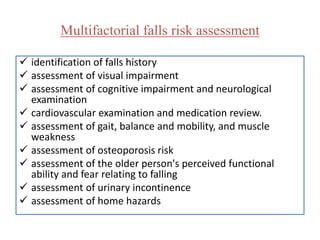
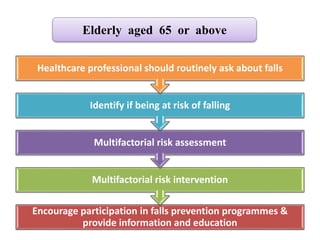
Falls are a common and serious problem for older adults. They can cause physical injuries like hip fractures as well as psychological issues like a fear of falling. A multifactorial assessment and intervention approach is recommended to prevent falls, which includes assessing vision, medications, home hazards, and exercise programs to improve balance and strength. Healthcare providers should routinely ask older patients about falls and recommend prevention strategies.





























































































![Session 6 se and complications [repaired]](https://cdn.slidesharecdn.com/ss_thumbnails/session6seandcomplicationsrepaired-180404084057-thumbnail.jpg?width=640&height=640&fit=bounds)

































