Download as PDF, PPTX
![References
Abigail L. Leddy, B. E. (2011, January). Functional Gait Assessment and Balance Evaluation System Test:
Reliability, Validity, Sensitivity, and Specificity, for Identifying Individuals With Parkinson Disease Who Fall.
Journal of the American Physical Therapy Association, pp. Vol 91, No. 1, pgs. 102-113.
Anne Shumway-Cook, M. B. (1997, August). Predicting the Probability for Falls in Community-Dwelling
Older Adults. Physical Therapy, Journal of the American Physical Therapy Association, pp. Vol. 77 No. 8 pgs.
812-819.
Barbara L. Fischer, C. E. (2014, March). Declining Cognition and Falls: Role of Risky Performance of
Everyday Mobility Activities. Journal of the American Physical Therapy Association, pp. Vol. 94, No. 3, pgs
355-362.
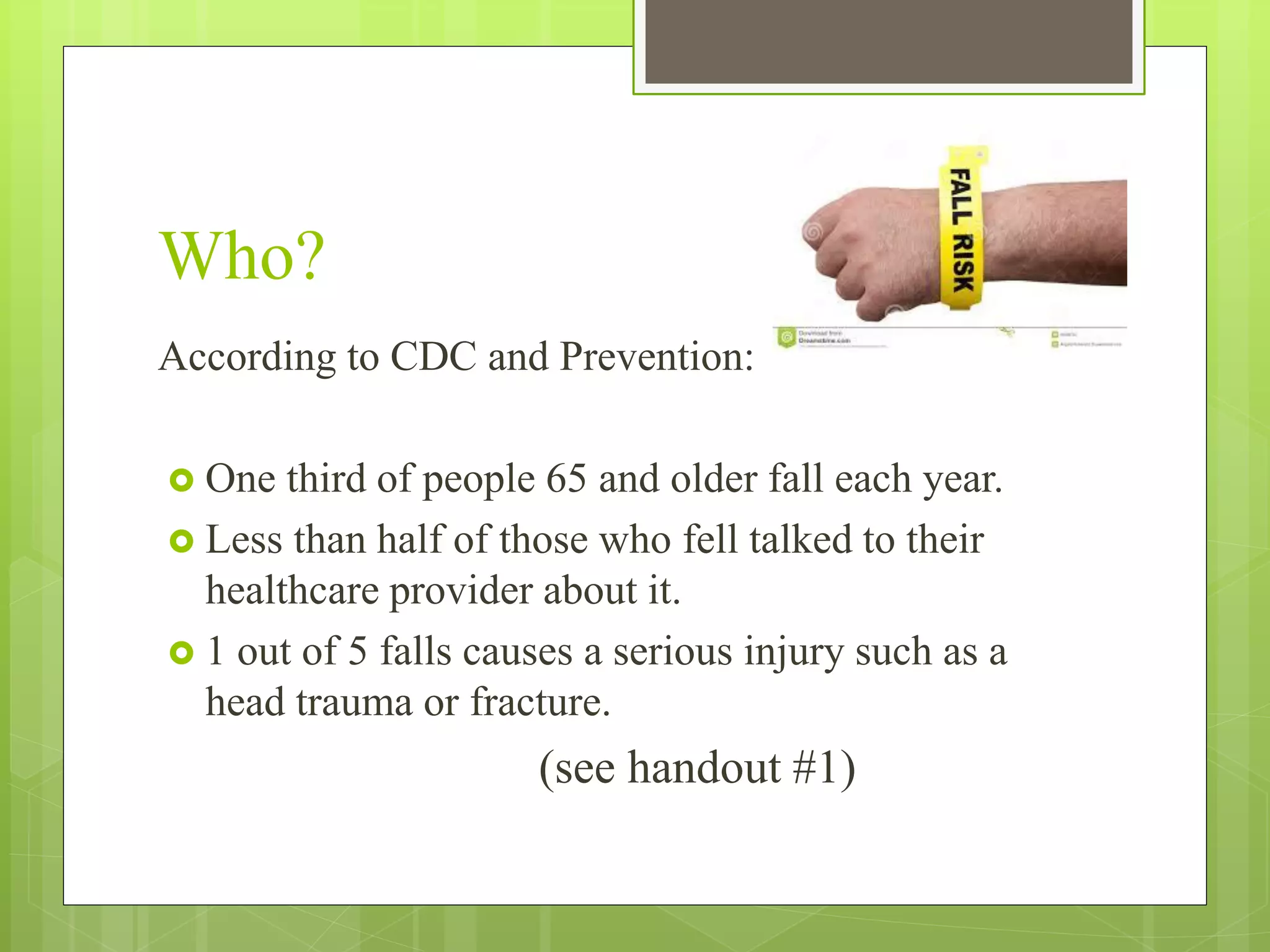
Centers for Disease Control and Prevention. National Center for Injury Prevention and Control (2014).
www.cdc.gov/injury/STEADI
Diane M. Wrisley, M. L. (2003, October). Reliability of the Dynamic Gait index in People with Vestibular
Disorders. Physical Medicine and Rehabilitation, pp. Vol. 84, Issue 10, pgs. 1528-1533.
Horak, M. M. (2010, June). The relevance of clinical balance assessment tools to differentiate balance deficits.
NIH Public Access. Eur J Phys Rehabil Med., pp. vol 46 No. 2: pgs 239-248.
Sara B. Vyrostek, J. L. (2004, September). Surveillance for Fatal and Nonfatal Injuries - United States, ,2001.
Morbidity and Mortality Weekly Report - Surveillance Summaries -MMWR, pp. Vol. 53/ SS-7 1-57.
Steffen T, Seney M. Test-retest Reliability and minimal detectable change on balance and ambulation tests, the
36-item short-form health survey, and the unified Parkinsons disease rating scale in people with parkinsonism
[erratum in Phys Ther. 2010;90:462]. Phys Ther. 2008;88:733-746](https://image.slidesharecdn.com/fallrisk-150529010444-lva1-app6891/75/Fall-risk-18-2048.jpg)

This document summarizes information from several sources about falls in older adults. It discusses statistics on falls from the CDC, including that one third of adults over 65 fall each year. It reviews assessment tools for evaluating fall risk such as the Berg Balance Scale, Dynamic Gait Index, and Timed Up and Go test. It also summarizes research studies on identifying fall risk factors and developing effective fall screening and prevention programs for older adult patients.
















































































![Apporach to lung biopsy [Auto-saved].pptx latest](https://cdn.slidesharecdn.com/ss_thumbnails/apporachtolungbiopsyauto-saved-251211225655-93258539-thumbnail.jpg?width=640&height=640&fit=bounds)