Fahr Syndrome- A Rare Case Report
•Download as PPTX, PDF•
4 likes•2,115 views

A 33-year-old female patient presented with complaints of loose teeth and was found to have oligodontia, gingival inflammation, and advanced periodontitis. She had a history of brain fever and meningitis as a child. Imaging found calcification in the basal ganglia consistent with Fahr syndrome. The patient was diagnosed with Fahr syndrome based on her clinical history and imaging findings. She received full-mouth tooth extraction and is undergoing dental rehabilitation.

Recommended
More Related Content
What's hot
What's hot (20)
Viewers also liked
Viewers also liked (20)
Similar to Fahr Syndrome- A Rare Case Report
Similar to Fahr Syndrome- A Rare Case Report (20)
More from Dr Gauri Kapila
More from Dr Gauri Kapila (12)
Recently uploaded
Recently uploaded (20)
Fahr Syndrome- A Rare Case Report
- 1. Gauri Kapila MDS student Department of Periodontology and Oral Implantology
- 2. A33-year-old female patient reported to the Department of Periodontics, Oxford Dental College, Bangalore, India, in May 2013 with the complaint of loose maxillary and mandibular teeth. Mobility was noticed 6 months previously > gradually increased > associated with pain and difficulty when eating. Written informed consent was obtained for additional examination and treatment on the same day.
- 3. The patient had normal growth and development until the age of 4 years, at which time the patient experienced brain fever and meningitis. This was followed by altered development, including stunted height, altered gait, and slow speech and learning. After the treatment for brain fever and meningitis, the patient had no history of epilepsy or any other health problems. The patient attained puberty at a normal age and reported a history of regular menstrual cycles.
- 4. Figure 1 illustrates patient’s short stature (141 cm height) Figure 2 shows the short digits on the hands and feet. The patient weighed 34.7 kg and had a spastic gait and poor motor coordination.
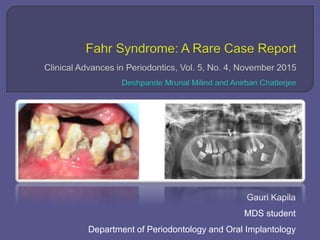
- 5. Figure 3 illustrates the oral findings, which include oligodontia with only 13 teeth present. The missing teeth included teeth #2, #6 through #11, #14 through #19, #22 through #27, #30, and #32. The gingiva of the remaining teeth was reddish-pink in color, soft, and edematous in nature, with increased size and absent stippling. Generalized bleeding on probing, generalized Miller Class IV recession, and Glickman Grade III mobility were noted.
- 6. A panoramic radiograph and cone-beam computed tomography (CBCT) of the maxilla and mandible showed a generalized advanced horizontal bone loss involving the alveolar and basal bones (Figs. 4 and 5).
- 7. After additional investigation, routine blood examination showed all the parameters within normal range, except hemoglobin (9 mg/dL), red blood cells (3.2 million/m), and packed cell volume (29%). Other blood investigations revealed that alkaline phosphatase (83 U/L) and triiodothyronine (168 ng/dL) levels were normal.
- 8. The thyroxine level (12.5 mg/dL) was slightly elevated (normal is 4.5 to 12 mg/dL), but the thyroid stimulating hormone level (7.44 mIU/L) was markedly elevated. The bone mineral density was low (SD of 2.4), indicating osteoporosis and increased risk of fracture. Considering the history of brain fever, stunted growth, and poor motor coordination, a CT scan of the brain was advised.
- 9. The CT scan showed areas of hyperdensity, indicating the presence of calcification of the basal ganglia (Fig. 6).
- 10. These findings are in accordance with the diagnostic criteria for Fahr syndrome, which include bilateral calcification of the basal ganglia as visualized on neuroimaging. There was an absence of biochemical abnormalities, and any infectious, toxic, or traumatic causes were ruled out. Meningitis does have neurologic manifestations, but they are not always present, and these neurologic symptoms in the patient are a result of bilateral calcifications seen in the basal ganglia. Saleem S, Aslam HM, Anwar M, et al. Fahr’s syndrome: Literature review of current evidence. Orphanet J Rare Dis 2013;8:156.
- 11. Based on the above findings, the authors, along with the physician (Dr. G. M. Arvind, Manipal Hospital, Bangalore, India), neurologist (Dr. E. V. Joshy, Sri Sai Hospital, Bangalore, India), and neuroradiologist (Dr. Zarina Aziz, Sri Sai Hospital), arrived at a diagnosis of Fahr syndrome. Full-mouth extraction was completed, and replacement of the teeth (maxillary and mandibular dentures) is currently in progress.
- 12. Fahr syndrome was first noted by the German neurologist Karl Theodor Fahr in 1930. It is a rare degenerative neurologic disorder characterized by calcifications and cell loss within the basal ganglia. The calcium deposits in the brain may occur before the onset of the symptoms, usually in the third decade of life. Fahr syndrome can be sporadic or familial and demonstrates no abnormalities in calcium metabolism and kinetics. Ogi S, Fukumitsu N, Tsuchida D, Uchiyama M, Mori Y, Matsui K. Imaging of bilateral striopallidodentate calcinosis. Clin Nucl Med 2002;27:721-724. Amin OS. Fahr’s disease: A case series. CukurovaMed J 2013;38:823-831.
- 13. Fahr syndrome is characterized by clinical heterogeneity and can be asymptomatic (frequent among middle-aged patients) or associated with neuropsychiatric manifestations. The true prevalence is unknown, but an incidence of basal ganglia calcifications ranging from 0.24% to 2% was reported in consecutive radiologic studies, showing an evident relationship with increasing age. Manyam BV. What is and what is not “Fahr’s disease.” Parkinsonism Relat Disord 2005;11:73-80.
- 14. Tedrus et al. reported an incidence of 0.68% among 3,662 cranial CT scans analyzed. Although bilateral and symmetric basal ganglia calcification is known to be associated with multiple medical conditions, the exact etiology is still unknown. Genetic alterations were attributed to genes in the region of chromosome 14. Tedrus GM, Fonseca LC, Nogueira EJ Jr. Basal ganglia calcification on computed tomography: Clinical characteristics in 25 patients (in Portuguese). Arq Neuropsiquiatr 2006;64:104-107.
- 15. Many of these conditions involve basal ganglia only or predominantly. The condition that was closely described with diffuse, bilateral, symmetric striopallidodentate calcinosis is primary hypoparathyroidism. When there is no explainable cause for striopallidodentate calcinosis, the condition is termed Fahr syndrome. Rastogi R, Singh AK, Rastogi UC, Mohan C, Rastogi V. Fahr’s syndrome: A rare clinico-radiologic entity. Med J Armed Forces India 2011;67:159-161.
- 16. According to Manyam et al. Fahr syndrome is found more often in males than in females, and movement disorders account for 55% of the total symptomatic patients. Most cases of Fahr syndrome present with extrapyramidal symptoms. Clinical expression of Fahr syndrome varies greatly. Symptoms include psychiatric disorders, epileptic seizures, and extrapyramidal syndrome and various neurologic conditions. Statistics showed that the prevalence of neurologic symptoms may vary in Fahr syndrome.
- 17. Oral examination of a patient with Fahr syndrome revealed oligodontia and Grade III mobility of the remaining teeth. Generalized gingival inflammation and Class III gingival recession was also seen. The patient in the current case report presented most of these symptoms, which are similar to those reported by Aditya et al.and Ahad et al.
- 18. The differential diagnosis considered was Hajdu-Cheney syndrome (HCS). The main clinical features of HCS include short stature, scoliosis and kyphosis, elongation of the skull, small chin, clubbing of the fingers, coarse hair, and thick eyebrows. Oral and dental manifestations of HCS are as follows: 1) premature exfoliation of the teeth; 2) dental maleruption and malocclusion; 3) increased tooth mobility; 4) impaction of teeth; 5) hypoplastic dental roots; 6) atrophy of the alveolar processes; and 7) structural changes in the dentin and cementum of teeth.
- 19. Radiographically, the most frequent findings include persistent wide cranial sutures, absence of the frontal and maxillary sinuses, and osteolysis of the distal phalanges. Another syndrome that can be considered for differential diagnosis is Kenny-Caffey syndrome, which is characterized by growth delay, cortical thickening of the long bones, hypocalcemia, hypothyroidism, and calcification of the basal ganglia. This was excluded in the current case because the majority of these features were absent in the patient.
- 20. Fahr syndrome is diagnosed based on clinical aspects, neuroimaging findings, and the exclusion of other primary causes. Final diagnosis in the present patient was given by the radiographic and laboratory findings and bilateral calcifications seen in the CBCT of the brain, specifically in the basal ganglia. Imaging also revealed progressive cerebral atrophy, pointing to a diagnosis of Fahr syndrome.
- 21. To the best of the authors’ knowledge, this is only the second case report that describes oral findings of a patient with Fahr syndrome. This case report will increase awareness of Fahr syndrome and help clinicians arrive at the correct diagnosis. Early presentation and diagnosis can help in early treatment and result in less mortality and morbidity
- 22. Fahr's disease with oral manifestations: report of a rare case. Aditya A, Lele S, Aditya P., 2012 CLINICAL PRESENTATION AND INTERVENTION: A patient presented with the complaint of partial anodontia, but further clinical and radiographic investigations showed a myriad of findings including stunted growth, osteoporosis and pathological calcifications. Oral findings included oligodontia and advanced periodontitis in relation to the present teeth. Full-mouth rehabilitation was eventually planned for the patient. CONCLUSION: This case shows the necessity for dentists to be aware of symptoms associated with Fahr's syndrome in order to make appropriate referrals and to enable diagnosis and treatment.