Presentation1, radiological imaging of wernicke encephalopathy.
•Download as PPTX, PDF•
13 likes•2,500 views

Wernicke encephalopathy is caused by thiamine (vitamin B1) deficiency and is commonly seen in alcoholics. On MRI, it shows symmetrical increased signal in the mammillary bodies, dorsomedial thalami, tectal plate, periaqueductal area, and around the third ventricle. The document discusses the clinical presentation and risk factors of Wernicke encephalopathy and provides examples of MRI and CT images demonstrating its characteristic radiological findings. It concludes that knowledge of the neuroimaging patterns can help make an early diagnosis to reduce morbidity and mortality.

Recommended
More Related Content
What's hot
What's hot (20)
Similar to Presentation1, radiological imaging of wernicke encephalopathy.
Similar to Presentation1, radiological imaging of wernicke encephalopathy. (20)
More from Abdellah Nazeer
More from Abdellah Nazeer (20)
Recently uploaded
Recently uploaded (20)
Presentation1, radiological imaging of wernicke encephalopathy.
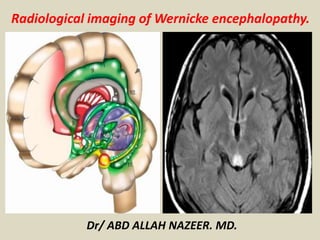
- 1. Radiological imaging of Wernicke encephalopathy. Dr/ ABD ALLAH NAZEER. MD.
- 2. Wernicke encephalopathy, also referred as Wernicke-Korsakoff syndrome, is due to thiamine (vitamin B1) deficiency, and is typically seen in alcoholics. On imaging, it is commonly seen on MRI as areas of symmetrical increased T2/FLAIR signal involving the mammillary bodies, dorsomedial thalami, tectal plate, periaqueductal area, and around the third ventricle. Clinical presentation It was originally described as characterised by the triad of: Acute confusion. Ataxia. Ophthalmoplegia. Wernicke encephalopathy can evolve into the chronic form of thiamine deficiency known as Korsakoff psychosis, characterised by: Memory loss (global amnesia). Confabulation. The two terms are often concatenated to form Wernicke-Korsakoff syndrome.
- 3. Aetiology Thiamine deficiency results from malnutrition or malabsorption, which can occur for a number of reasons: Alcohol abuse (up to 90% in industrialized countries) Starvation/fasting. Prolonged total parental nutrition without supplementation. Post bariatric surgery. Hyperemesis gravidum. Gastrointestinal malignancy. Chronic dialysis.
- 4. Radiographic features CT usually normal MRI T2/FLAIR: symmetrically increased signal intensity in the: mammillary bodies dorsomedial thalami tectal plate periaqueductal area around the third ventricle T1 C+ (Gd): contrast enhancement can also be seen in the same regions, most commonly of the mamillary bodies DWI/ADC: restricted diffusion can also be seen in the same regions MR spectroscopy: may show decreased or normal NAA with the notable presence of lactate
- 5. Midsagittal T2-weighted MR image with gray-scale inversion in healthy 37- year-old man shows schematic representation of anatomic regions typically (circles) and infrequently (asterisks) affected by Wernicke's encephalopathy. Note that caudate capita and dentate nuclei are not seen in this view.
- 6. 33-year-old man affected by acute Wernicke's encephalopathy caused by severe malnutrition.
- 7. A 54-year-old woman with leukemia, changes in consciousness, and ataxia. FLAIR axial images (11,000/140/2 [TR/TE/NEX]). A, The prepositus hypoglossal nuclei show symmetric high-signal-intensity alterations (arrows). B, The medial vestibular nuclei show symmetric hyperintense lesions (arrows). C, Symmetric high-signal-intensity alterations in the facial nuclei (arrows) are detected. Subtle signal-intensity alterations in the abducens nuclei are seen (arrowheads). D, The tectum of the midbrain and the periaqueductal gray matter shows signal-intensity alterations (arrow). E, The mamillary bodies (arrows) show signal-intensity alterations. F, Note signal-intensity alterations (arrows) of the medial thalami and periventricular region of the third ventricle.
- 8. A 54-year-old woman with a history of food refusal had changes in consciousness. FLAIR coronal images (11,000/140/2 [TR/TE/NEX]). A, Signal-intensity alterations with different intensity patterns are seen in the thalami (arrows). Diffuse signal-intensity alterations of the frontal cortex (arrowheads) are present. B, Note signal-intensity alterations in the mamillary bodies (arrows), periventricular region of the third ventricle (empty arrows), and brain cortex (arrowheads).
- 9. Wernicke encephalopathy With bilateral thalami abnormal signal and restricted diffusion.
- 10. CT and MRI images of 35 year-old man with schizophrenia and acute nutritional deficiency-induced WE. CT. T2- weighted late- echo fast spine echo image. Fluid-attenuated inversion recovery image. Diffusion-weighted image.
- 11. Typical MR findings of acute Wernicke Encephalopathy Fluid-attenuated inversion recovery images presenting symmetric high-signal intensity alterations in the mammillary bodies and colliculi (a), periventricular gray matter (b), and fornix and thalamus (c).
- 12. Wernicke Encephalopathy: MRI in a sixteen weeks pregnant woman with recent mental status change, repeated vomiting, and weight loss. Axial FLAIR shows abnormal bright signal.
- 13. Hemorrhagic Wernicke encephalopathy In a patient with liver transplantation.
- 14. A, The prepositus hypoglossi nuclei regions show symmetric high signal-intensity alterations (arrows). B, The abducens nuclei regions show symmetric hyperintense alterations (black arrows). Symmetric high signal-intensity alterations in the facial nuclei (white arrows) are seen. C, The tectum of the midbrain and the periaqueductal gray matter demonstrates signal-intensity alterations (black arrows). Focal lesions in the medial lemniscus are seen bilaterally (white arrows). D, The inferior quadrigeminal plate, the periaqueductal gray matter (black arrows), and the corticospinal tracts (white arrows) show contrast enhancement. E, Signal-intensity alterations of the mamillary bodies are detected (white arrows). F and G, Symmetric alterations of the posterior putamen (white arrows) and periventricular region of the third ventricle (black arrows) are seen on fluid-attenuated inversion recovery and diffusion-weighted images, respectively. H, Signal-intensity alterations are seen in the motor strip (arrows).
- 15. T2-weighted images show the high signal intensities in the bilateral paramedian thalami with mamillary bodies (A) and in the periaqueductal gray matter (B). Diffusion-weighted images show the bright high signal intensities in the corresponding lesions (C and D). The corresponding apparent diffusion coefficient values of the lesions range from 512 to 545 × 10−6mm2/s.
- 16. Changes on MRI with Wernicke's encephalopathy.
- 17. Magnetic resonance images in a patient affected by alcoholic Wernicke’s encephalopathy. A-D: MR images before intravenous administration of thiamine therapy; E-H: MR images after intravenous administration of thiamine therapy. Axial FLAIR images (A,B) and DWI images (C,D) show signal abnormalities in the periaqueductal area and in the medial thalami. Axial FLAIR (E,F) and DWI (G,H) follow-up MR images, after intravenous administration of thiamine therapy, show resolution of the signal abnormalities previously observed. MR: Magnetic resonance; FLAIR: Fluid-attenuated inversion recovery; DWI: Diffusion weighted image.
- 18. Wernicke-Korsakoff syndrome in a nonalcoholic patient: (A) Gadolinium-enhanced T1-weighted axial MRI shows symmetric enhancement of the mamillary bodies (paired arrowheads). (B) Enlarged axial view of the region of the hypothalamus showing mamillary body enhancement (paired arrowheads). (C) Enlarged coronal view of the mamillary body enhancement (paired arrowheads). (D) FLAIR hyperintensity of the hypothalamus is seen in an axial view (arrows). (E) FLAIR hyperintensity of the periaqueductal gray (arrows). (F) FLAIR hyperintensity of the dorsomedian thalamus (arrows). (G) FLAIR hyperintensity of the floor of the fourth ventricle (arrows). (H) FLAIR hyperintensity is seen throughout the low medulla (arrows).
- 20. Alcoholic 65 years-old patient with Wernicke’s encephalopathy. There are symmetrical hyperintense lesions on these axial T2-WIs in the paraventricular regions of the thalamus and hypothalamus, periaqueductal regions of the midbrain, and floor of the fourth ventricle
- 21. Symmetrical hyperintense lesions on these axial FLAIR images in the paraventricular regions of the thalamus and hypothalamus and periaqueductal regions of the midbrain.
- 22. 33-year-old woman, primipara, in her 16th week of gestation: coronal FLAIR (a) and sagittal T2-weighted (b) MR images showing bilateral and symmetric hyperintense signal alteration at the level of the medial portion of the thalami and of the tectal plate.
- 23. Wernicke encephalopathy in a 29-year-old woman who had severe hyperemesis gravidarum throughout pregnancy. Axial fluid-attenuated inversion-recovery and Diffusion weighted MR image shows bilateral symmetrical FLAIR hyperintensity with some diffusion restriction in dorsomedial thalami, mammillary bodies and periaqueductal grey (arrows)
- 24. CONCLUSION. Wernicke's encephalopathy is characterized by a quite distinct pattern of MR alterations, which include symmetrical alterations in the thalami, mamillary bodies, tectal plate, and periaqueductal area, but atypical alterations may also been seen. A thorough knowledge of the neuroimaging findings of Wernicke's encephalopathy will assist in arriving at an early diagnosis, thus reducing the morbidity and mortality associated with this disease.
- 25. Thank You.