This document provides information on the facial nerve (cranial nerve VII) including its embryology, anatomy, functions, and various disorders. It discusses the facial nerve's motor and sensory roles. Disorders covered include Bell's palsy, Ramsay Hunt syndrome, Moebius syndrome, and Guillain-Barré syndrome. Classification systems for facial nerve paralysis and nerve injuries are also summarized. The document provides detailed information on evaluating facial nerve disorders.
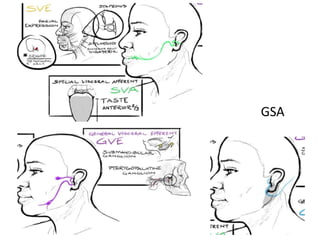
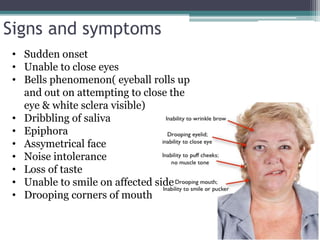
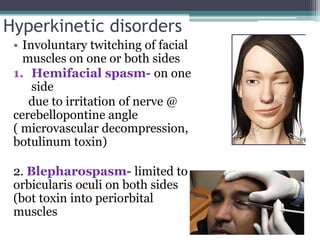
![• Unilateral facial weakness
• Loss of taste
• Hyper acusis
• Vesicles in the ear(shingles)
• Facial pain]
• decreased salivation
• Decreased tear secretion](https://image.slidesharecdn.com/facialnerveanditsdisorders-161207105113/85/Facial-nerve-and-its-disorders-15-320.jpg)