Downloaded 293 times



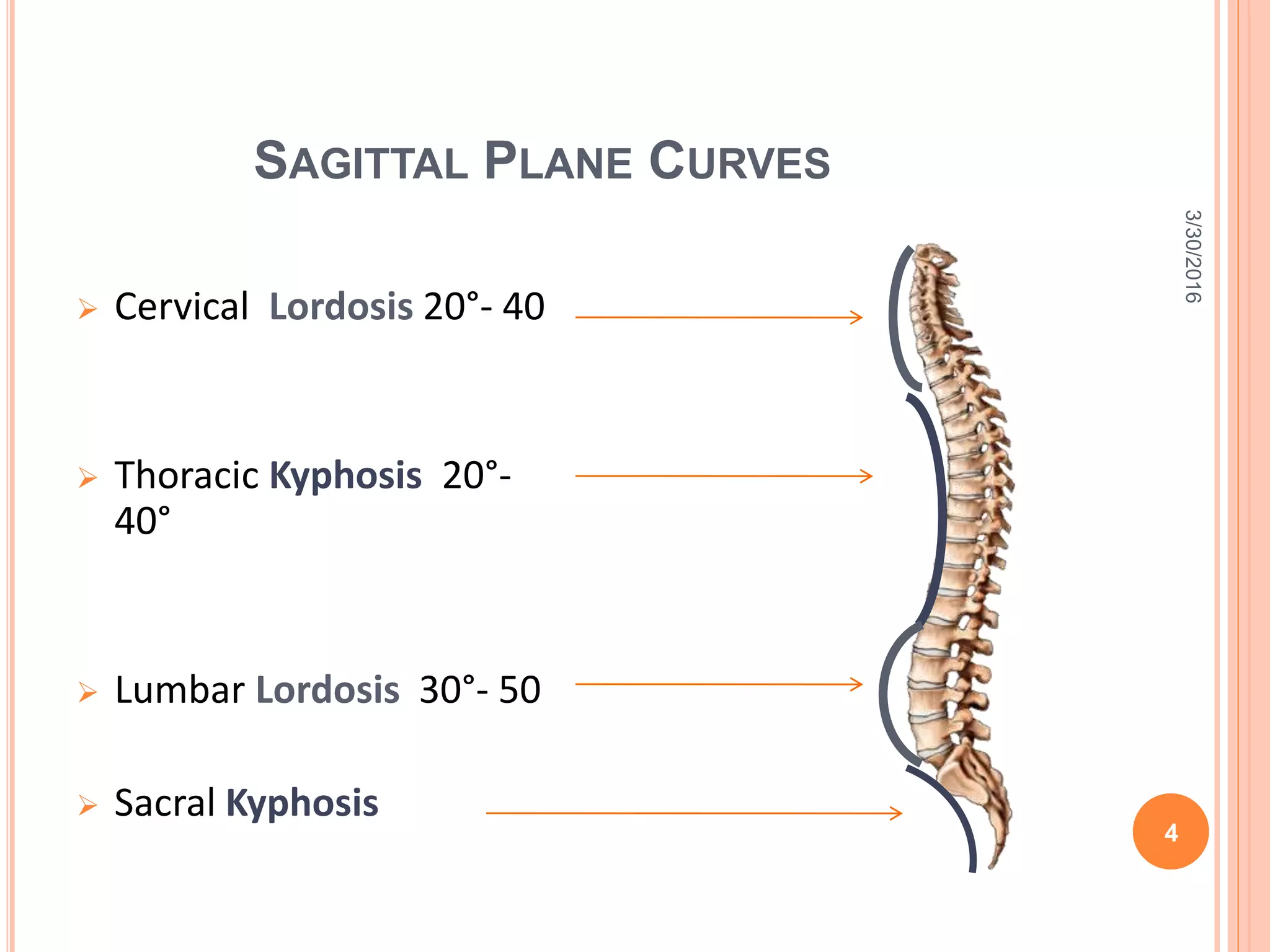
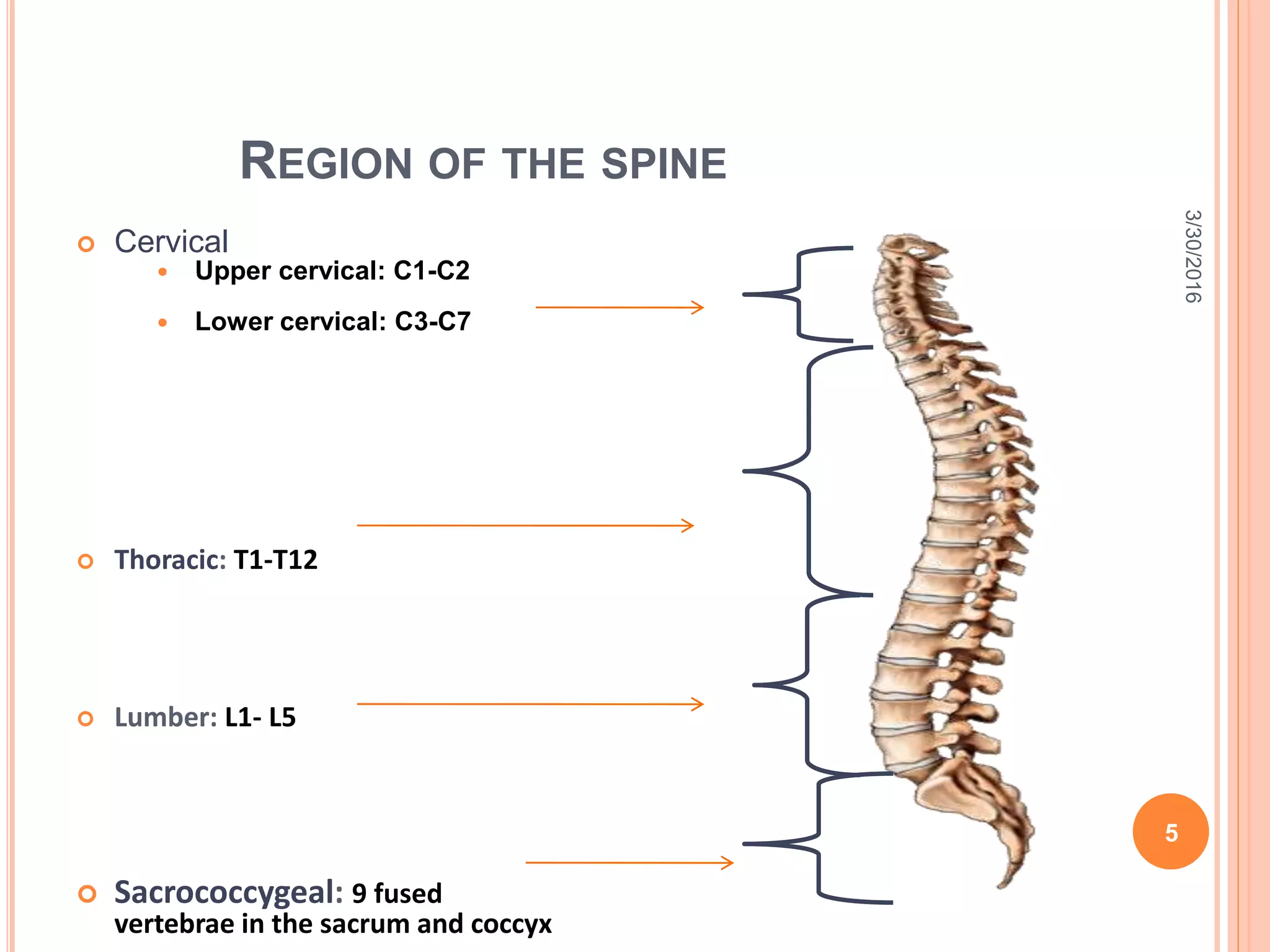

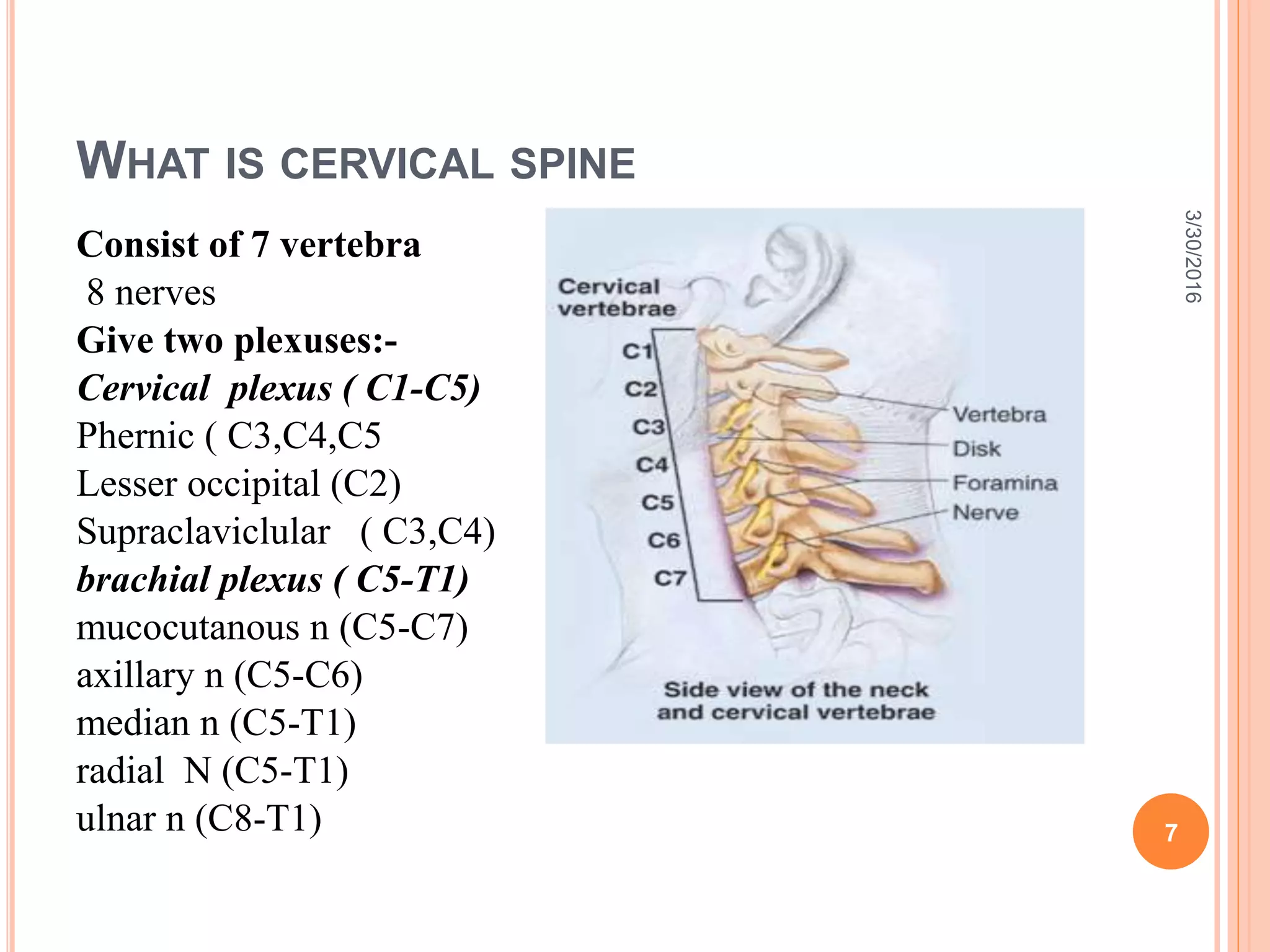
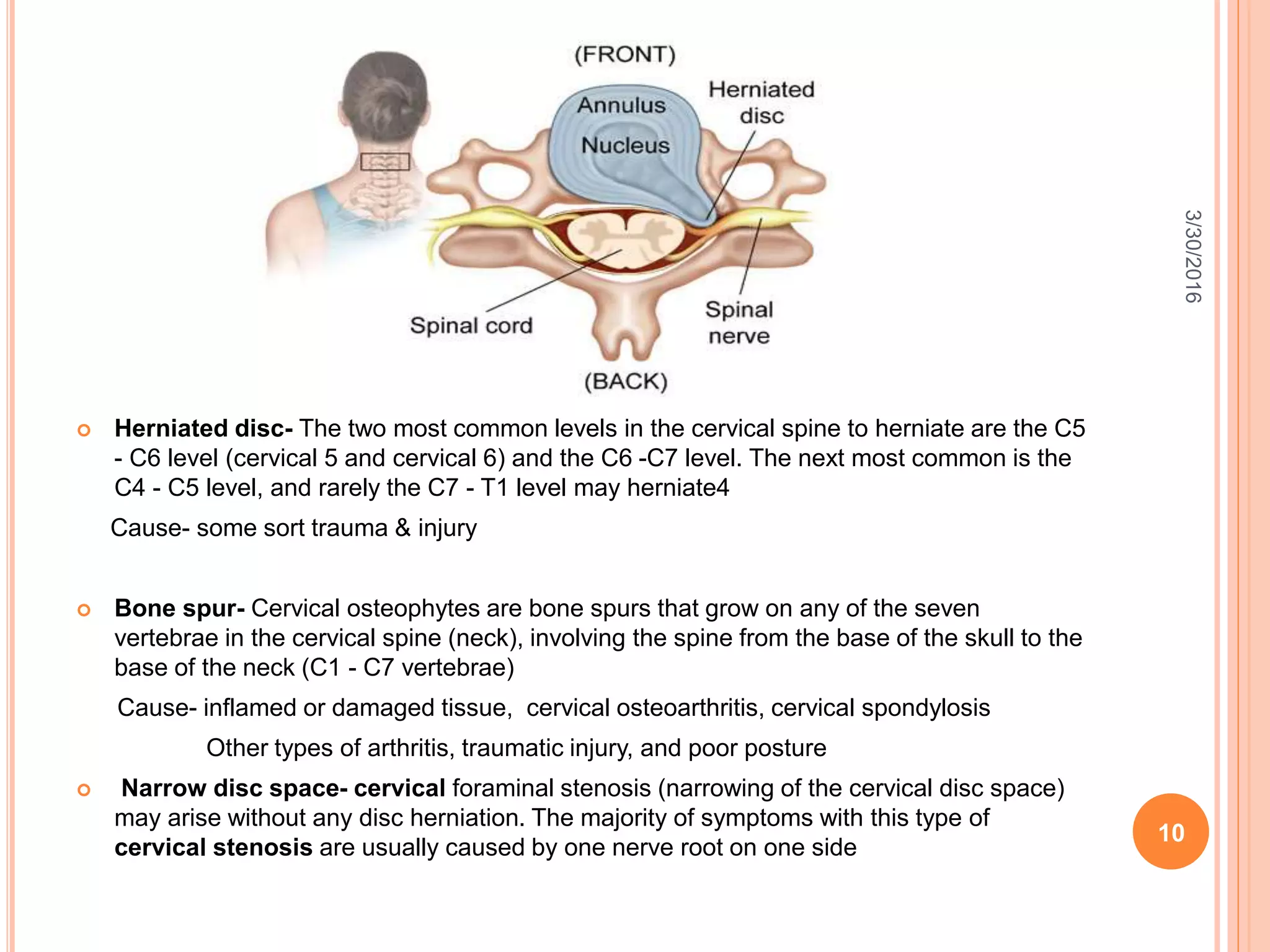






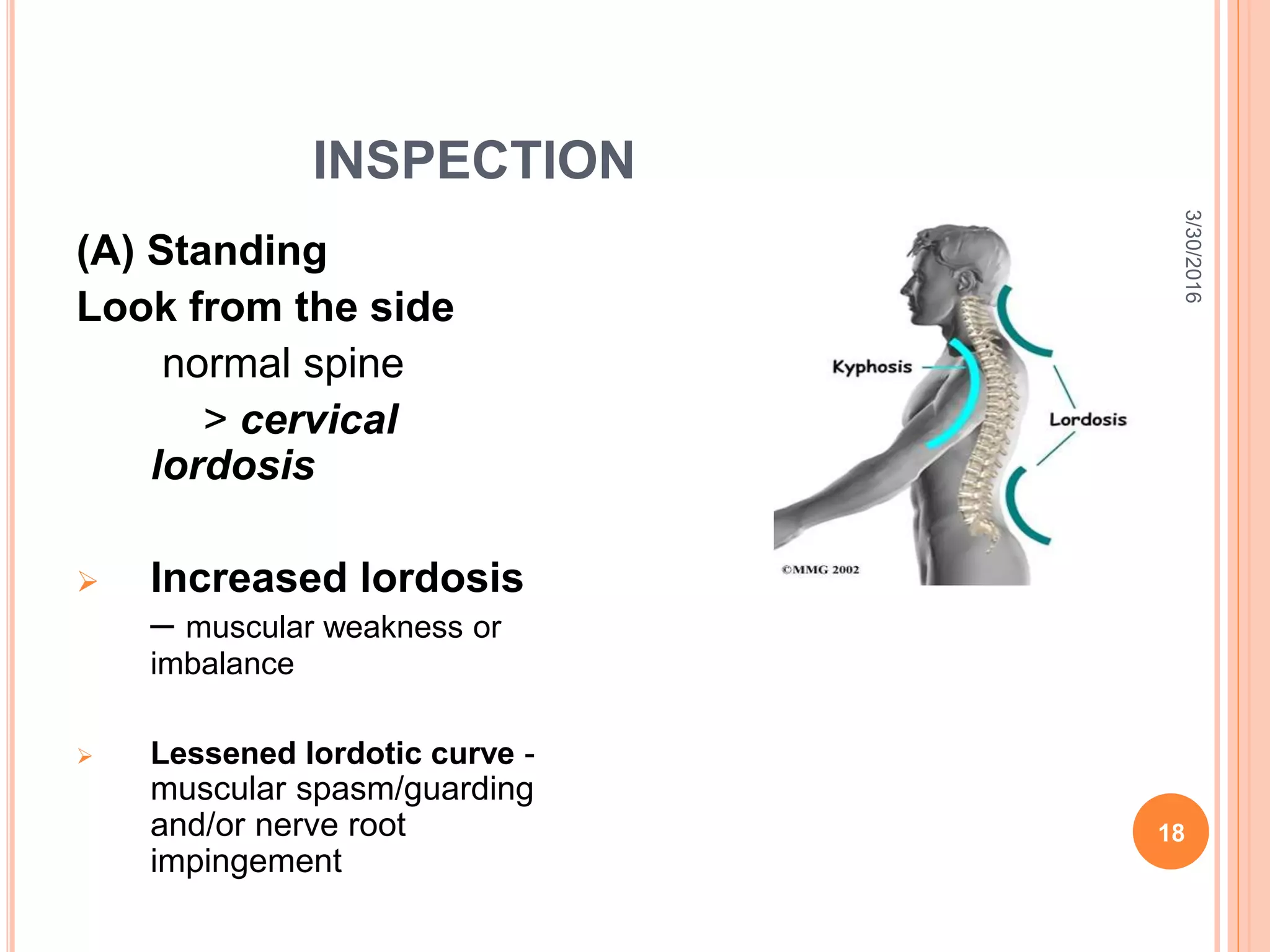











The document discusses the examination of cervical disorders. It begins with an introduction to the anatomy of the cervical spine and then describes the various functions of the spine. The document outlines the process for examining the cervical spine, including obtaining a history, inspecting for abnormalities, palpating the spine, and performing special tests to assess range of motion and potential nerve impingement. Common cervical conditions like herniated discs and bone spurs are also summarized. The examination techniques are explained in detail with diagrams to illustrate proper procedures like compression, distraction, and rotation tests.