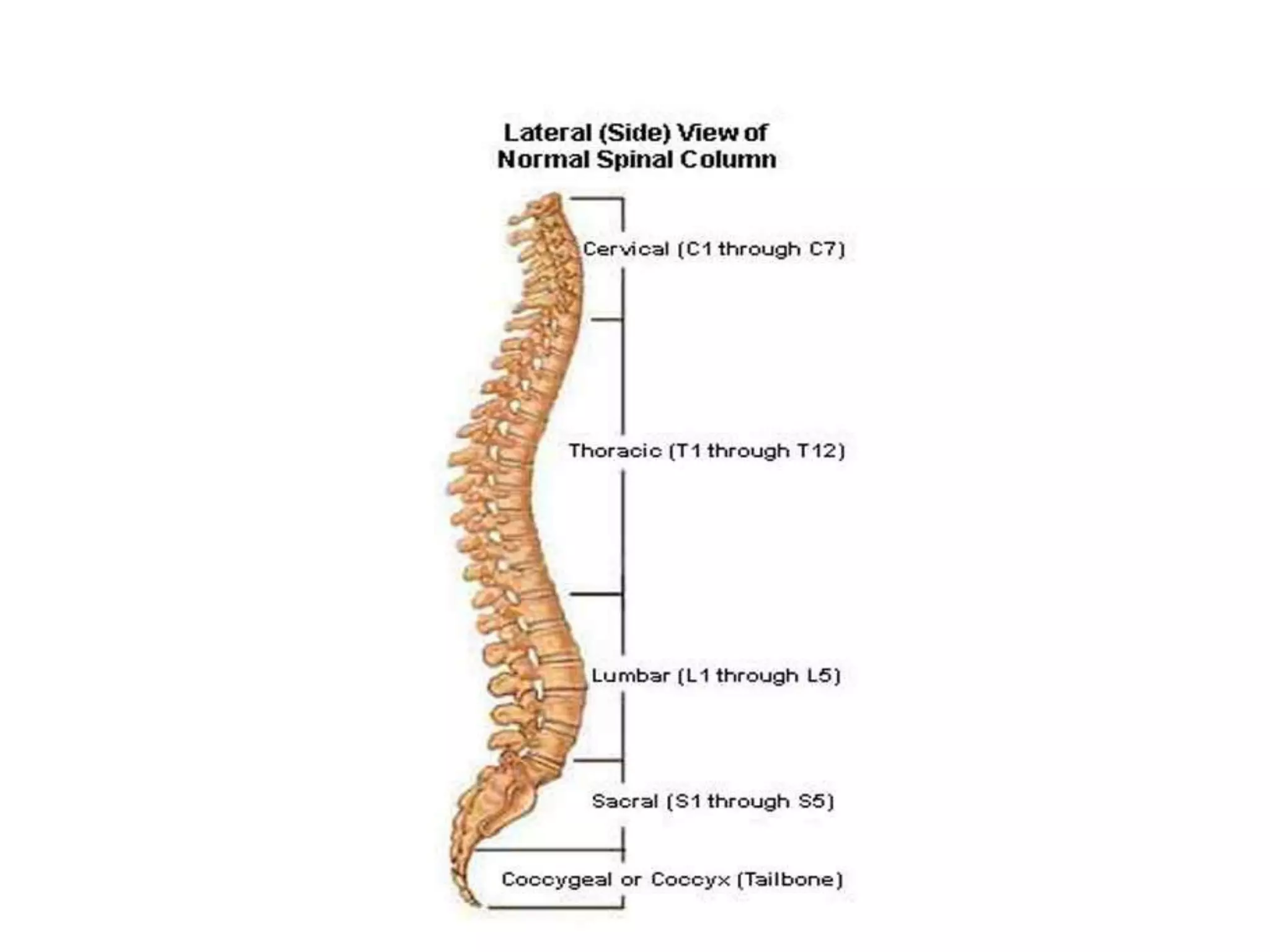
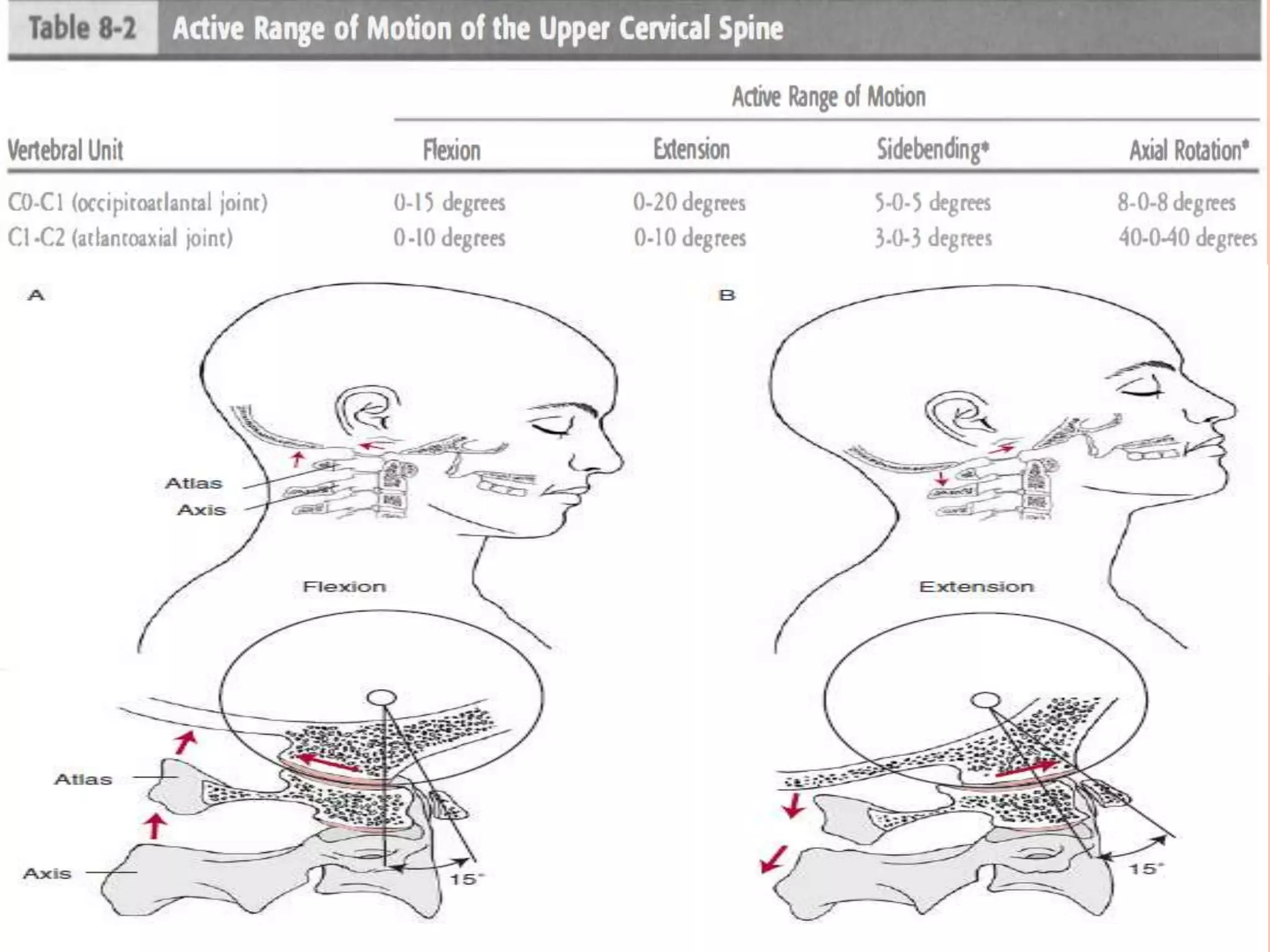
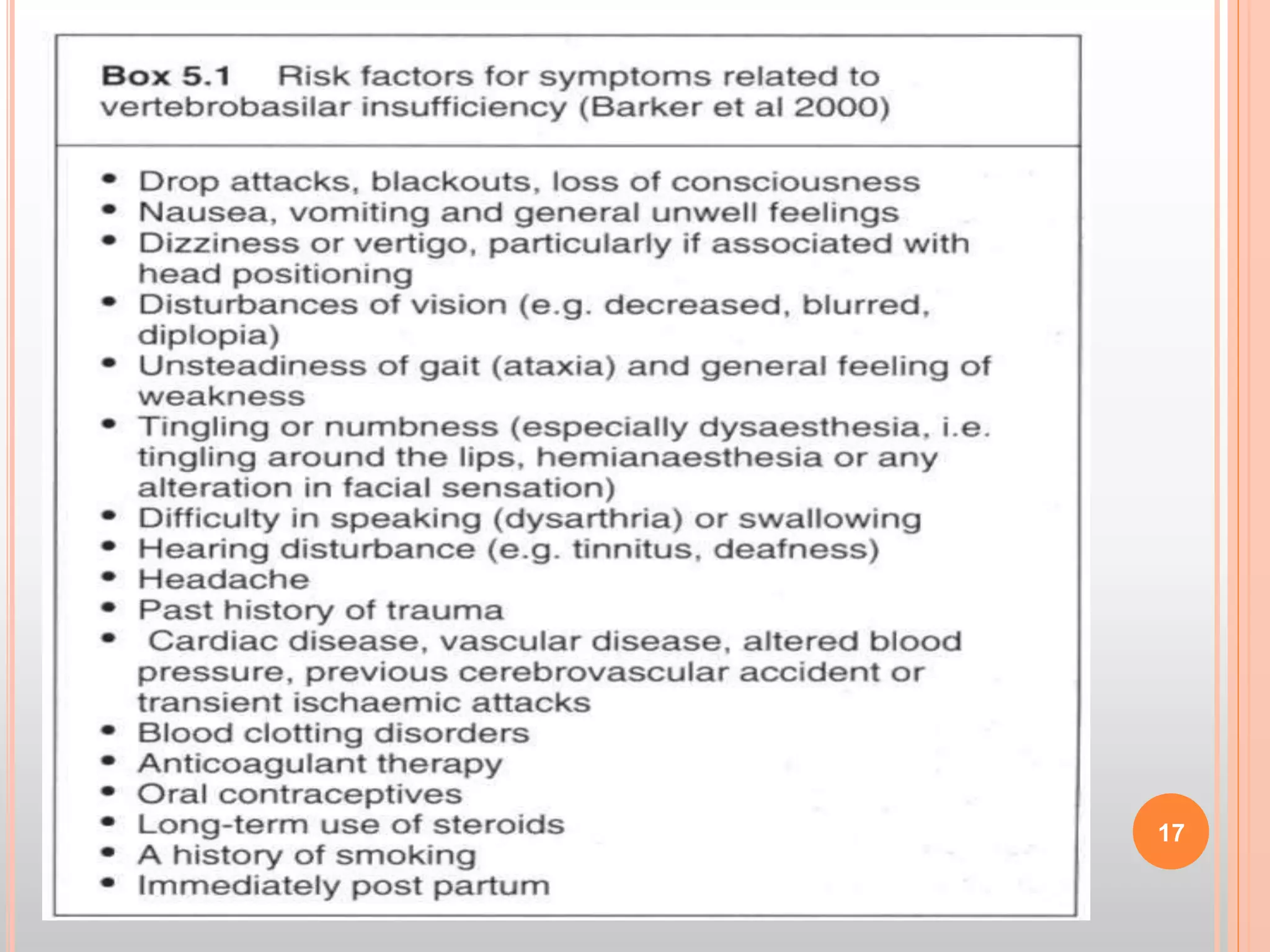
This document provides information about conducting a subjective cervical spine examination. It discusses the anatomy of the cervical spine, possible causes of cervical pain, and components of the subjective examination. The subjective examination includes using a body chart to document the location, quality, and characteristics of pain. It also involves asking special questions about symptoms like dizziness and assessing factors like aggravating activities, easing techniques, and how symptoms impact daily living. The goal is to gather detailed self-reported information from the patient to guide the physical examination and evaluation of their cervical condition.