Downloaded 425 times
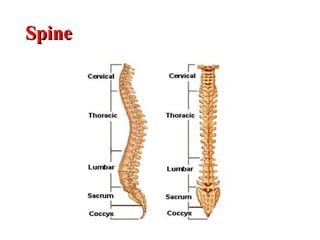
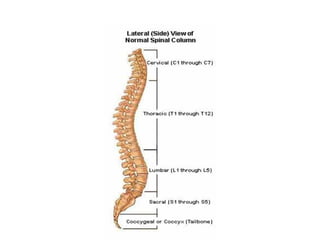
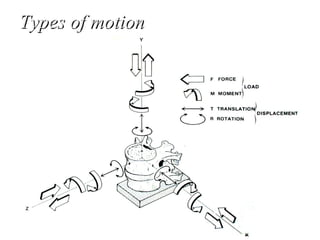
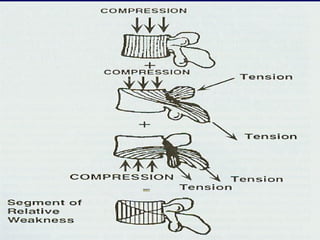
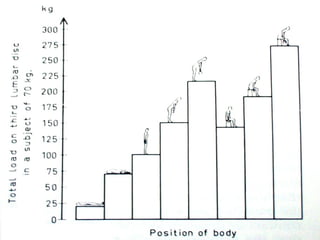
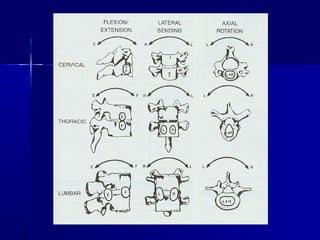
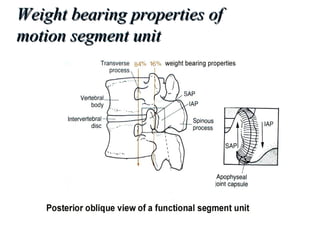
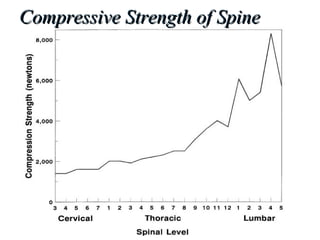

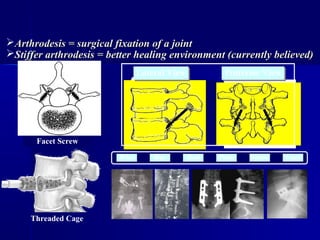

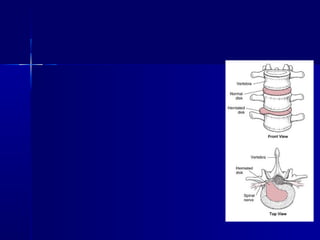


This document discusses spine biomechanics, describing the anatomy and motions of the cervical, thoracic, lumbar, and sacral regions. Key points include that the cervical spine has 7 vertebrae and a wide range of motion including rotation and flexion. The thoracic spine is rigid and immobilized by the attachment of ribs. The lumbar spine carries the weight of the upper body and has large flexion-extension motion. Compressive loads are highest in the center of vertebral endplates.

















































![MT-01 Anatomy and biomechanics of cervical spine-102024 [Autosaved].pptx](https://cdn.slidesharecdn.com/ss_thumbnails/mt-01anatomyandbiomechanicsofcervicalspine-102024autosaved-250827121120-fd4fe0b6-thumbnail.jpg?width=640&height=640&fit=bounds)











































