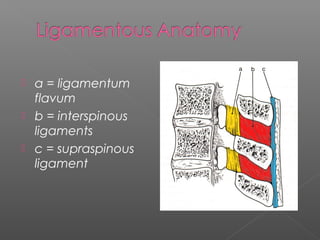
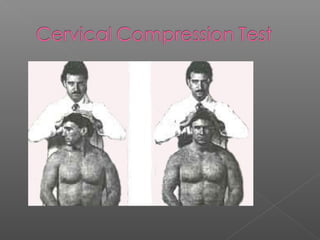
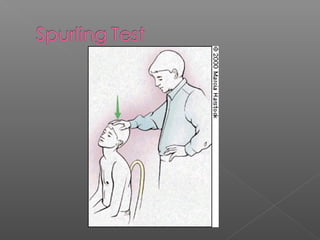
This document discusses cervical spine anatomy, injuries, and evaluation. It outlines the ligaments of the cervical spine, dermatomes, myotomes, and common mechanisms of injury. It provides details on evaluating range of motion, neurological function, and special tests like Spurling's test and brachial plexus traction test to assess for cervical injuries. Treatment options depend on the specific vertebrae and type of fracture, ranging from bracing to surgery.