Downloaded 41 times
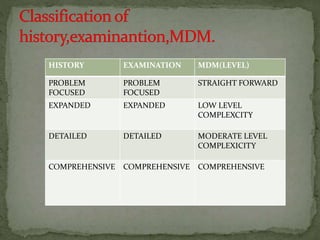

The document discusses evaluation and management (E/M) coding guidelines. It covers the key components of E/M codes which are history, examination, and medical decision making. E/M codes are used to bill for office visits, hospital visits, consultations, and other services. Assignment of the codes depends on factors like new vs. established patient, type of service, place of service, patient age, and time spent. History, examination, and medical decision making are the three main components used to determine the level of E/M service provided.









![Evaluation_and_Management[1]](https://cdn.slidesharecdn.com/ss_thumbnails/8209e160-4c89-43f5-bde3-1a2ee8242cc6-150226150420-conversion-gate01-thumbnail.jpg?width=640&height=640&fit=bounds)




























































































