LEARNING OUTCOMES
After studyingthis chapter, you should be able to:
1. Explain the purpose of the CPT code set.
2. Identify the medical settings in which CPT is used.
3. Describe the content and organization of CPT.
4. Identify the symbols, format and punctuation used in CPT.
5. Discuss the purpose and use of CPT modifiers, distinguishing
among CPT professional, HCPCS, and facility modifiers.
6. Recognize the importance of using current codes and discuss
ways to stay up to date.
7. Compare and contrast the ICD-9-CM and CPT code sets.
8. List CPT coding resources and references.
9. Recognize when an unlisted code is needed, and identify the
purpose and parts of a special report.
10. List the nine steps to properly assign CPT codes and to correctly
select and append modifiers.
2
3.
DESCRIPTION OF CPT
•CPT is a coding nomenclature that allows
medical procedures to be transformed to
numbers
• CPT is based on professional services provided
by healthcare providers such as physician,
nurse practitioners and physician assistants
• CPT services include office visits, surgery,
laboratory, radiology, pathology, anesthesia and
medical procedures
3
4.
CPT BACKGROUND
• CPTwas developed by the American Medical
Association (AMA) in 1966.
• CPT is still currently maintained by the AMA
• CPT code sets
– HCPCS level I (Healthcare Common Procedure Coding
System)
• CPT codes maintained by AMA
– HCPCS level II
• HCPCS codes maintained by Federal Government
4
5.
PURPOSE OF CPT
•Reimburse physician services
• Trending services provided nationally
• Future coding and reimbursement planning
• Benchmarking facilities, costs and services
• Measuring quality of care and patient outcomes
nationally
5
6.
ALL CPT CODESMUST BE:
• Commonly performed by physicians across the
nation
• Consistent with mainstream medical practice
• Approved by the AMA CPT Editorial Board
6
7.
ORGANIZATION OF CPT
•Each code is followed by a unique code
descriptor explaining the service
• More than 8,000 unique CPT codes
• CPT codes are 5 digits long
• CPT manual includes parenthetical notes
7
8.
INTRODUCTION TO CPT
•Category I codes are permanent codes
• 6 Sections of Category I codes-each with a set
of guidelines at the section beginning
– Evaluation and Management (E/M)
– Anesthesia
– Surgery
– Radiology
– Pathology/Laboratory
– Medicine
8
9.
EVALUATION AND MANAGEMENT
SECTION
•Code Ranges 99201 - 99499
• Cover physician services that are performed to
determine the best course for patient care
9
10.
ANESTHESIA SECTION
• CodeRanges 00100 – 01999
• Used to report anesthesia services performed or
supervised by a physician
• Codes include routine anesthesia care
– Pre-op, intra-op, post-op
10
11.
SURGERY SECTION
• Largestsection in the CPT book
• Code ranges 10021 – 69990
• Divided by body systems
– Integumentary, musculoskeletal, respiratory,
digestive, cardiology, urinary, male/female, nervous,
auditory/ocular
• Codes are for a surgical package
– Pre-op, intra-op, post-op
11
12.
RADIOLOGY SECTION
• CodeRanges 70010 – 79999
• Used to report radiological services performed
or supervised by a physician
• Codes are selected based on the body part and
number/type of view
12
13.
PATHOLOGY/LABORATORY SECTION
• CodeRanges 80048 – 89356
• Cover services provided by physicians or
technician supervised by physicians
• Complete procedure includes:
– Ordering the test
– Taking/handling the sample
– Performing the test
– Analyzing/reporting on the test results
13
14.
MEDICINE SECTION
• CodeRanges 90281 – 99607
• Codes include the many types of evaluation,
therapeutic, and diagnostic procedures that
physicians/health care providers perform
• May be used by procedures done or supervised
by a physician of any specialty
14
15.
CATEGORY II CODES
•Used to track physician performance in
measuring and monitoring patient care
• Are alphanumeric codes, start with 1 letter then
followed by 4 numbers
• Improve quality of care but are not “billable”
15
16.
CATEGORY III CODES
•Introduced in 2002
• They are used to report new technology,
services or procedures that do not currently
have a CPT code assigned
• Located directly after the Category II codes
• Allow researchers to track emerging technology
16
17.
APPENDIXES
• Appendix A
–Lists/examples of modifiers
• Appendix B
– Summary of additions/deletions/revisions
• Appendix C
– Clinical Examples of E/M Codes
• Appendix D
– Summary of CPT Add-on Codes
17
18.
APPENDIXES CONTINUED
• AppendixE
– Summary of CPT codes exempt from -51
• Appendix F
– Summary of CPT codes exempt from -63
• Appendix G
– Summary of CPT codes which include conscious
sedation
• Appendix H
– Alphabetical index of performance measures by
clinical condition or topic
18
19.
APPENDIXES CONTINUED
• AppendixI
– Genetic Testing Code Modifiers
• Appendix J
– Electrodiagnostic Medicine Listing of Sensory, Motor
and Mixed Nerves
• Appendix K
– Product Pending FDA Approvement
• Appendix L
– Vascular Families
• Appendix M
– Crosswalk to deleted CPT codes
19
20.
PUNCTUATION AND SYMBOLS
;Semicolon
– Divides the common portion of a code descriptor from
the unique portion
• Bullet
– New Code
▲Triangle
– Revised code
+ Plus Symbol
– Add on code
20
21.
PUNCTUATION AND SYMBOLS
CONTINUED
Modifier 51 Exempt
– Indicates the code cannot be assigned with -51
►◄Facing Triangles
– That the code is new or revised since the last year’s
edition
Circled Bullet
– That conscious sedation is included in code
Lightning Bolt
– Is for a vaccine pending FDA Approval
21
22.
MODIFIERS
• 2-digit charactersadded to the end of a CPT
code
• Used to communicate special circumstances
surrounding the assigned code
• May increase or decrease the amount of
reimbursement
• Three types of modifiers
– CPT Modifiers
– Facility Modifiers
– HCPCS Modifiers
22
23.
CPT MODIFIERS
• Listedin the front cover of the CPT book
• List of these:
– 21 -22 -23 -24 -25 -26 -27 -32 -47 -50
– 51 -52 -53 -54 -55 -56 -57 -58 -59 -62
– 63 -66 -73 -74 -76 -77 -78 -79 -80 -81
– 82 -90 -91 -99
23
24.
FACILITY MODIFIERS
• Thereare 13 approved facility modifiers
• Some of these are the same of the CPT
modifiers
• List of these:
– 25 -27 -50 -52 -58 -59 -73
– 74 -76 -77 -78 -79 -91
24
25.
HCPCS MODIFIERS
• Arealphanumeric
• Some are in the front of the CPT book and the
remaining are in the HCPCS book
• Required when filing claims to government
payors
• List of these:
– Ca -E1 -E2 -E3 -E4 -FA -F1 -F2 -F3 -F4
– F5 -F6 -F7 -F8 -F9 -GA -GG -GH -LC
– LD -RC -QM -QN -TA -T1 -T2 -T3 -T4
– T5 -T6 -T7 -T8 -T9 -TC
25
26.
DESCRIPTION OF MODIFIERS
•-21 – prolonged evaluation and management services
• -22 – unusual (increased) procedural services
• -23 – unusual anesthesia
• -24 – unrelated evaluation and management service by
the same physician during a postoperative period
• -25 – significant, separately identifiable evaluation and
management service by the same physician on the same
day of the procedure or other service
• -26 – professional component
• -27 – multiple outpatient hospital E/M encounters on the
same date
• -32 – mandated services
• -47 – anesthesia by surgeon
• 50 – bilateral procedure
• 51 – multiple procedures
26
27.
DESCRIPTION OF MODIFIERS
•-52 – reduced services
• -53 – discounted procedure
• -54 – surgical care only
• -55 – postoperative management only
• -56 – preoperative management only
• -57 – decision for surgery
• -58 – staged or related procedure or service by the same
physician during the postop period
• -59 – distinct procedural service
• -62 – two surgeons
• -63 – procedure performed on infants less than 4 kg
• -66 – surgical team
• - 73 - discontinued out-patient hospital/ambulatory
surgery center procedure prior to the administration of
anesthesia
27
28.
DESCRIPTION OF MODIFIERS
•-74 - discontinued out-patient hospital/ambulatory
surgery center procedure after administration of
anesthesia
• -76 – repeat procedure by same physician
• -77 – repeat procedure by another physician
• -78 – return to the operating room for a related
procedure during the postoperative period
• -79 – unrelated procedure or service by the same
physician during the postoperative period
• -80 – assistant surgeon
• -81 – minimum assistant surgeon
• -82 assistant surgeon (when qualified resident surgeon
not available)
• - 90 – reference (outside) laboratory
• -91 – repeat clinical diagnostic laboratory test
• -99 – multiple modifiers
28
29.
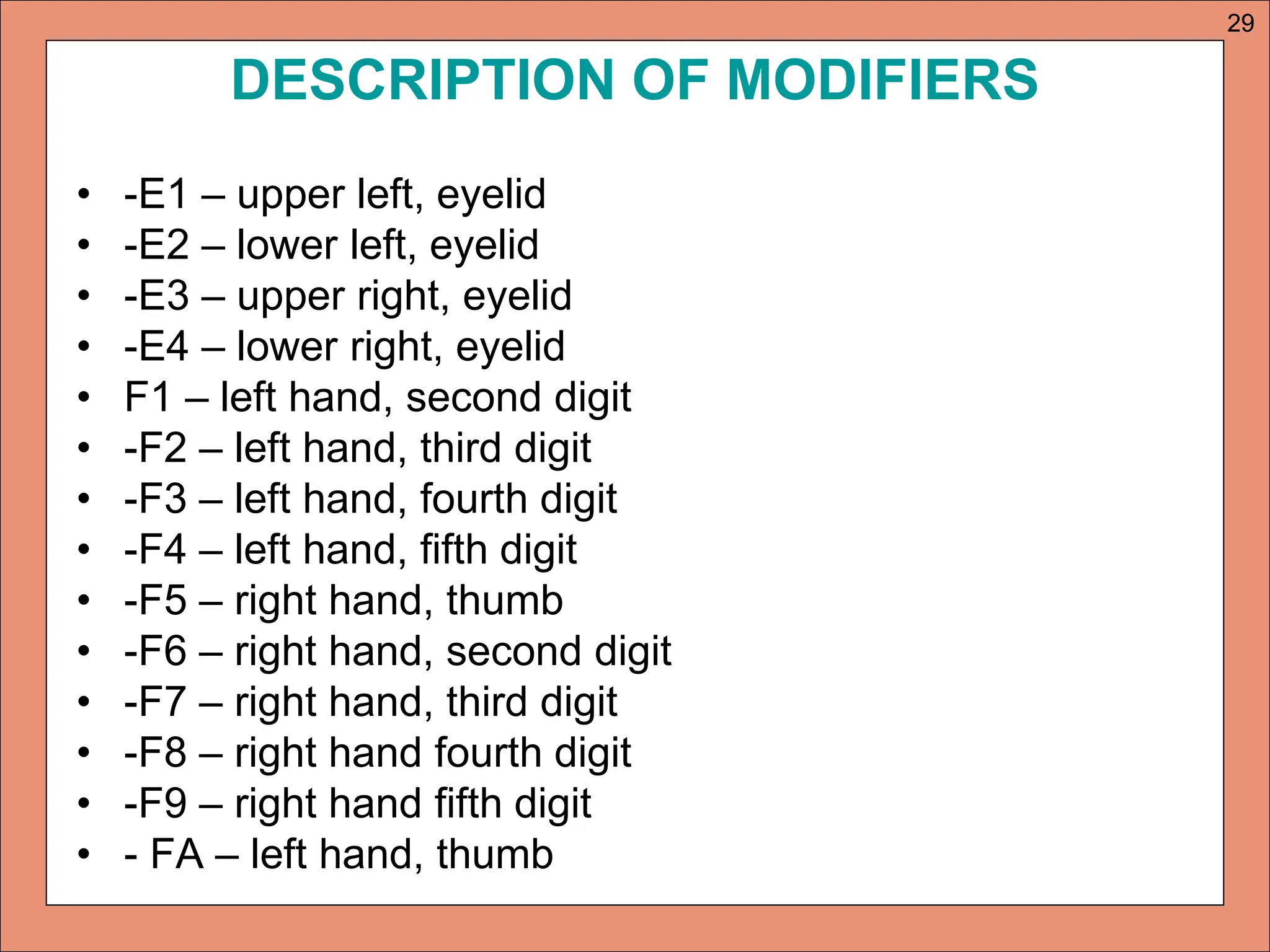
DESCRIPTION OF MODIFIERS
•-E1 – upper left, eyelid
• -E2 – lower left, eyelid
• -E3 – upper right, eyelid
• -E4 – lower right, eyelid
• F1 – left hand, second digit
• -F2 – left hand, third digit
• -F3 – left hand, fourth digit
• -F4 – left hand, fifth digit
• -F5 – right hand, thumb
• -F6 – right hand, second digit
• -F7 – right hand, third digit
• -F8 – right hand fourth digit
• -F9 – right hand fifth digit
• - FA – left hand, thumb
29
30.
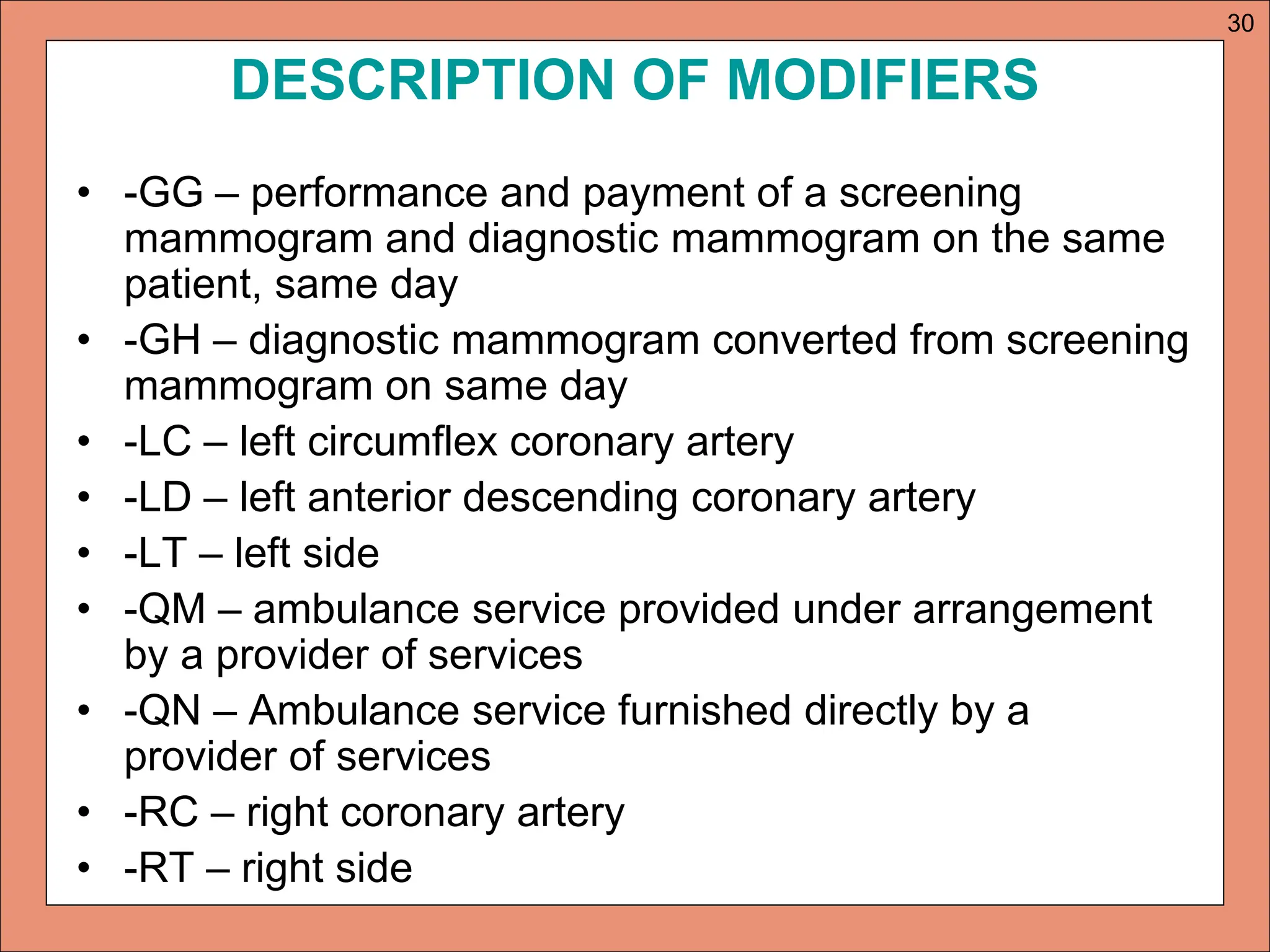
DESCRIPTION OF MODIFIERS
•-GG – performance and payment of a screening
mammogram and diagnostic mammogram on the same
patient, same day
• -GH – diagnostic mammogram converted from screening
mammogram on same day
• -LC – left circumflex coronary artery
• -LD – left anterior descending coronary artery
• -LT – left side
• -QM – ambulance service provided under arrangement
by a provider of services
• -QN – Ambulance service furnished directly by a
provider of services
• -RC – right coronary artery
• -RT – right side
30
31.
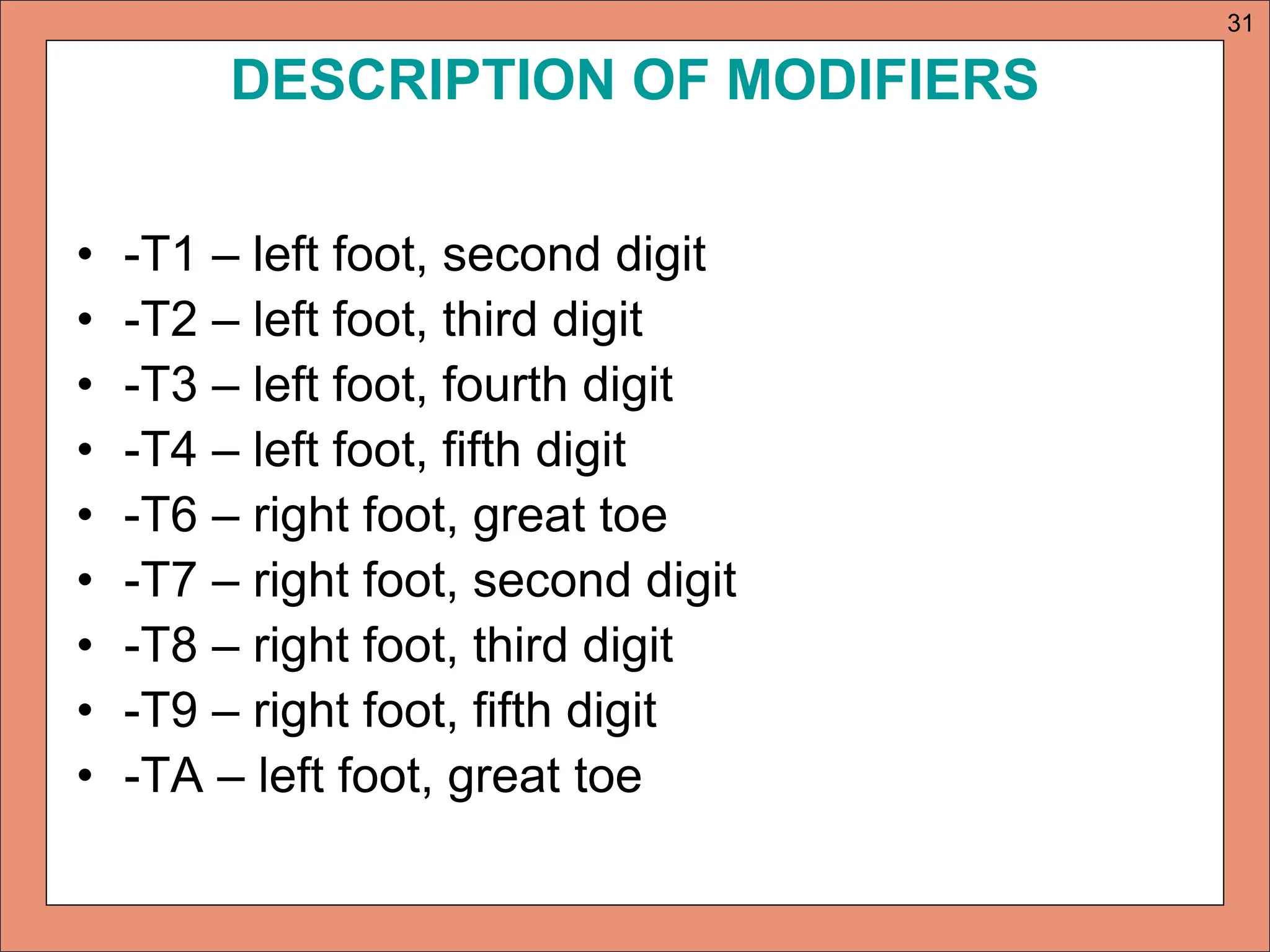
DESCRIPTION OF MODIFIERS
•-T1 – left foot, second digit
• -T2 – left foot, third digit
• -T3 – left foot, fourth digit
• -T4 – left foot, fifth digit
• -T6 – right foot, great toe
• -T7 – right foot, second digit
• -T8 – right foot, third digit
• -T9 – right foot, fifth digit
• -TA – left foot, great toe
31
32.
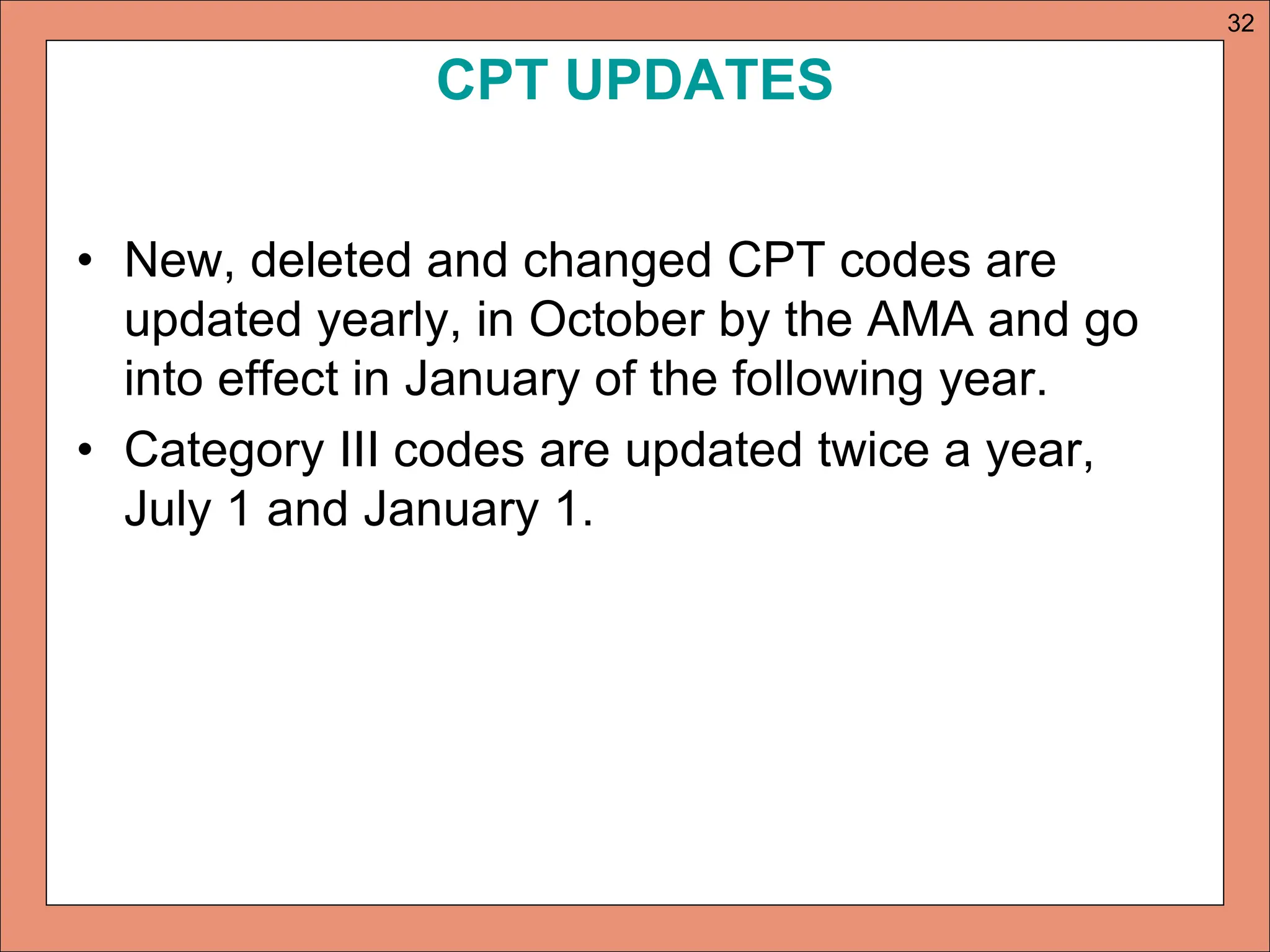
CPT UPDATES
• New,deleted and changed CPT codes are
updated yearly, in October by the AMA and go
into effect in January of the following year.
• Category III codes are updated twice a year,
July 1 and January 1.
32
33.
HOW TO ASSIGNCPT CODES AND
MODIFIERS
• Step 1: review the complete medical
documentation
• Step 2: Abstract the medical procedures that
should be coded
• Step 3: Identify the main terms and related terms
• Step 4: Locate the terms in the CPT index
• Step 5: Review the codes, descriptors and notes
33
34.
HOW TO ASSIGNCPT CODES AND
MODIFIERS
• Step 6: Verify the code against the
documentation
• Step 7: Assign codes for all significant services
• Step 8: Assign modifiers, if appropriate
• Step 9: Check all possibilities before final code
assignment
34
35.
HELPFUL CPT CODINGRESOURCES
• Medical Dictionary
• Anatomy & Physiology Text
• Current ICD-9-CM, CPT, and HCPCS codebooks
• Physician’s Desk Reference
• Merck Manual
• Contractor’s Provider Manual
• Subscription to AHA Coding Clinic
• Subscription to AMA Coding Assistant
• www.cms.hhs.gov/NationalCorrectCodInitEd
• www.cms.hhs.gov/center/coverage.asp
35