Download to read offline

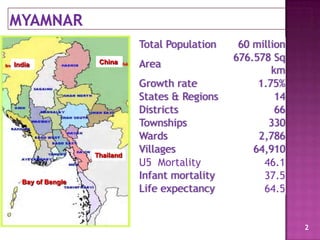


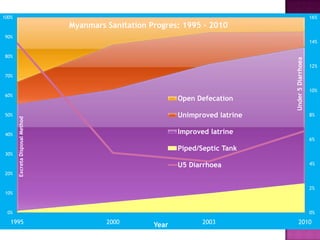
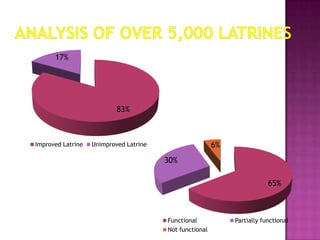

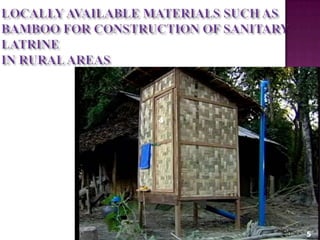


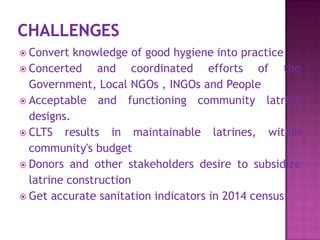

This document discusses Myanmar's sanitation progress and strategies. It provides an overview of the country's demographics and sanitation indicators. It then outlines Myanmar's sanitation approaches over time, shifting from supply-driven to demand-driven and introducing Community-Led Total Sanitation (CLTS) in 2011. The document details CLTS implementation methods and activities in Myanmar and pilot results in some townships. It recognizes challenges around sustainability and open defecation rates. The conclusion emphasizes continued efforts through the National Sanitation Campaign to achieve total sanitation coverage by 2015.











































































































