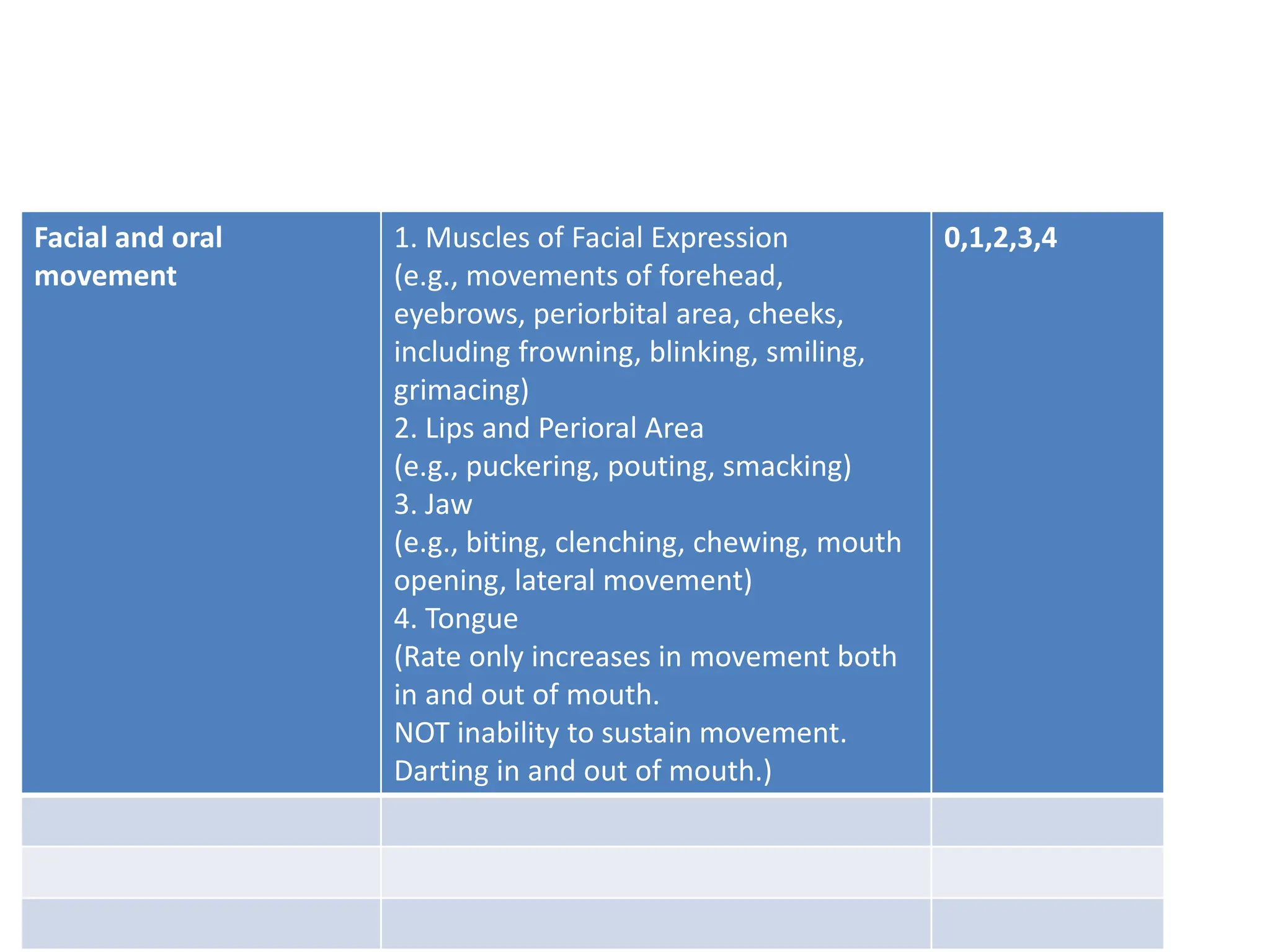
The document discusses extrapyramidal side effects (EPS) caused by antipsychotic medications, detailing definitions, symptoms, and treatment approaches for major types such as dystonia, akathisia, pseudo parkinsonism, and tardive dyskinesia. It emphasizes the importance of recognizing these symptoms as they can significantly impact patient well-being and may require prompt intervention. Additionally, the document introduces the Abnormal Involuntary Movement Scale (AIMS) for assessing the severity of these movements.