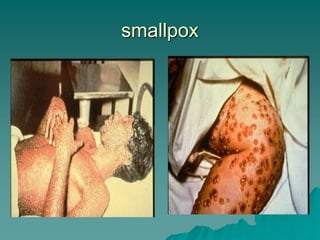
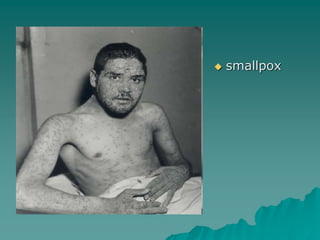
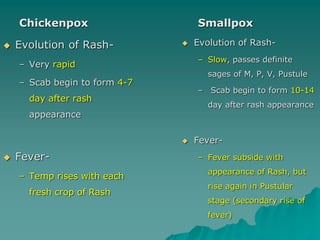
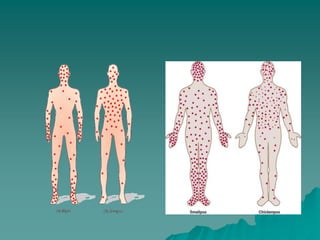
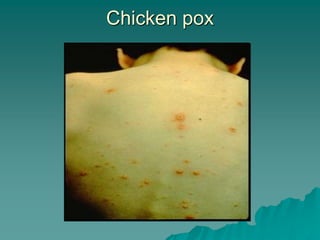
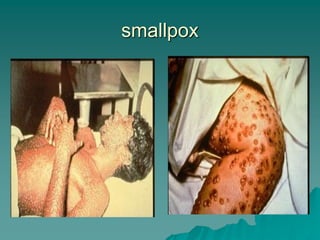
Smallpox was the first disease to be eradicated globally through vaccination efforts. The last case was reported in Somalia in 1977. Smallpox vaccination led to the prevention of millions of deaths and cases of blindness. While smallpox virus samples are still maintained in laboratories in the US and Russia, smallpox outbreaks pose little threat today due to widespread immunity in populations from previous vaccination programs. Chickenpox, caused by the varicella zoster virus, is a highly contagious disease typically affecting children under 10 years old and causing a rash that spreads from the trunk to the face and extremities.