This document defines endometriosis and discusses its causes, sites, types, clinical presentation, investigations, management, and prophylaxis. The key points are:
1. Endometriosis is defined as the presence of endometrial tissue outside the uterus, which responds to hormones in a cyclical manner.
2. Theories for its causes include retrograde menstruation, coelomic metaplasia, and genetic factors.
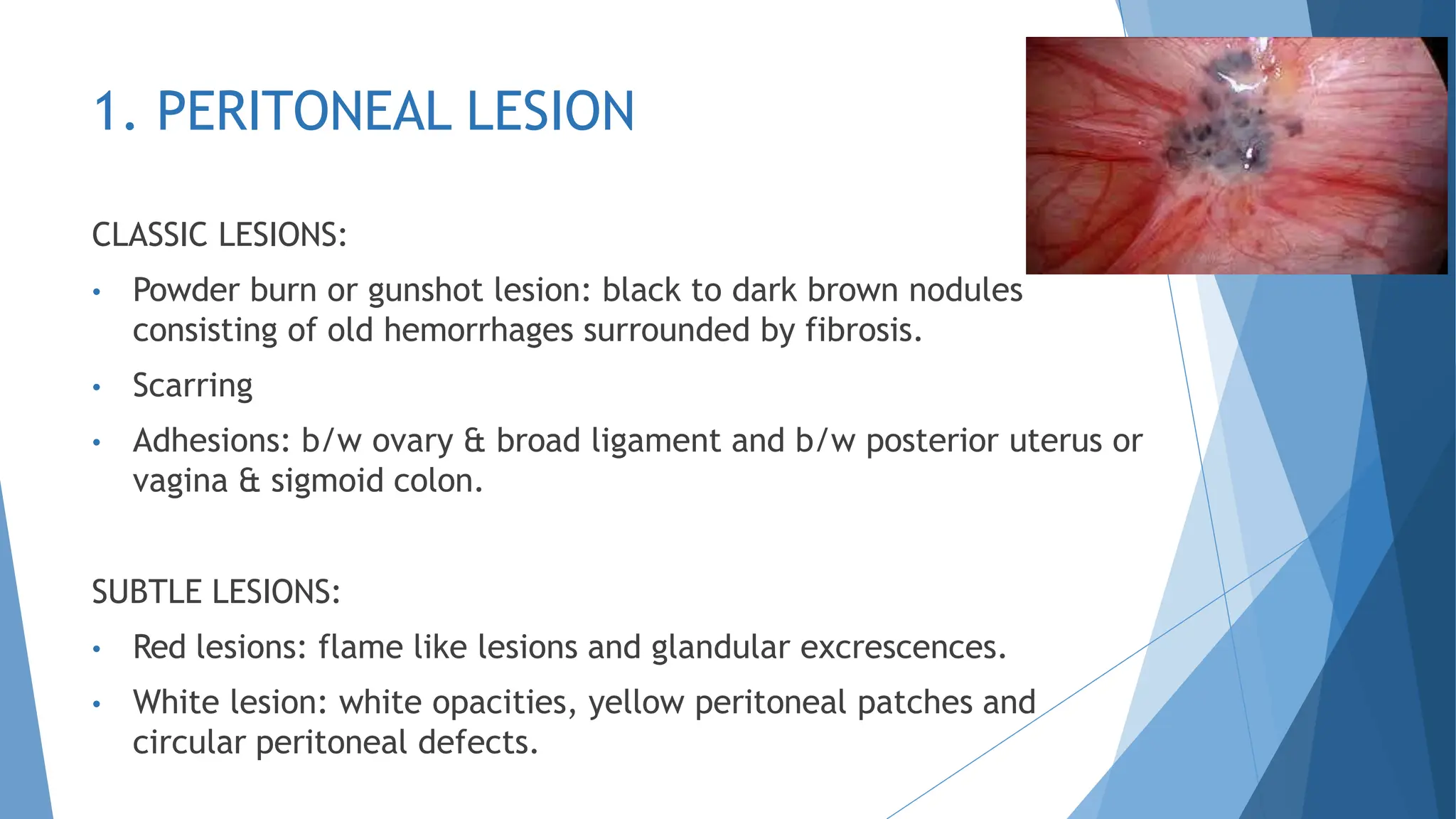
3. It commonly involves the ovaries, peritoneum, and deep infiltrating tissues in the pelvis. Symptoms include pelvic pain and infertility.
4. Diagnosis involves medical history, physical exam, ultrasound, laparoscopy and biopsy of