Downloaded 11 times










![The Key
• Push hard [to 2 inches]
• Push Fast [100 per minute]
• Recoil [get your hands off]
• And
• Don’t Stop [for 2 minutes]](https://image.slidesharecdn.com/ctexpo-150601173921-lva1-app6892/85/CT-EMS-EXPO-SCA-SYSTEMS-36-320.jpg)
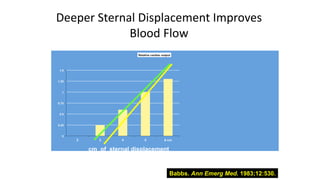
![• The deeper you compress the higher the cardiac output. The
key is 5 cm, 2 inches, even in children [the AHA states that in
children compressions should be 1/3 the AP diameter of the
chest approximately 2 inches!].](https://image.slidesharecdn.com/ctexpo-150601173921-lva1-app6892/85/CT-EMS-EXPO-SCA-SYSTEMS-40-320.jpg)
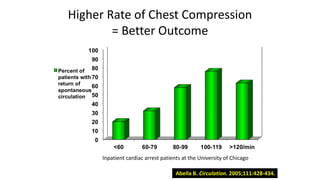
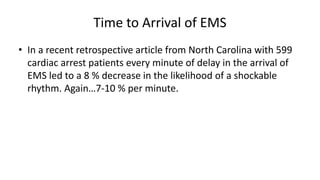
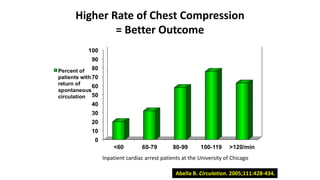
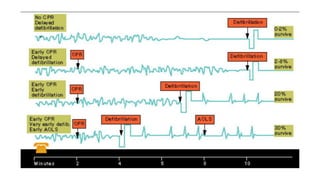
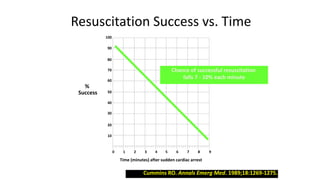
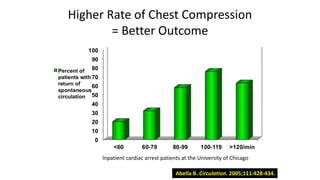
![The Key on Rate
• The previous slide , from an ICU in Chicago , reveals 2 things , one is
that ROSC [return of circulation, and therefore survival ] is directly
related to the rate. The ROSC at a rate of 60 compressions per
minute is only ¼ as high as the rate of ROSC at 100 compressions
per minute.
• The other very important bit of data is that when the compression
rate exceeds 120 the rate of ROSC declines. You must maintain a
rate of 100.](https://image.slidesharecdn.com/ctexpo-150601173921-lva1-app6892/85/CT-EMS-EXPO-SCA-SYSTEMS-43-320.jpg)
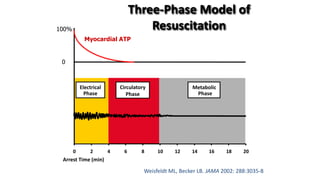
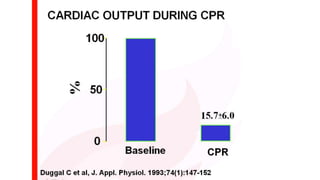
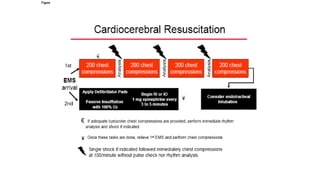
![The Key [again]
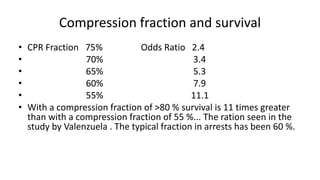
• The previous slide makes it clear that the compression fraction ,
how continuous your chest compressions are, determine your
survival. If your compression fraction is >80 % your survival is 11
times more likely than with a compression fraction of 55 %
[essentially , you are compressing only half the time ]. This slide
basically shows a straight line of survival with the continuity of
chest compressions . DON’T STOP CHEST COMPRESSIONS. They are
the patients only heart beats.](https://image.slidesharecdn.com/ctexpo-150601173921-lva1-app6892/85/CT-EMS-EXPO-SCA-SYSTEMS-47-320.jpg)
![Get Your Hands off the chest and ALLOW RECOIL
Blood flow to the coronary arteries only occurs in diastole. Diastole occurs
when the heart is relaxing and is finished with its compression. This
corresponds to when you let up from a chest compression, “RECOIL”. If you
maintain your hands on the chest during recoil there is inadequate blood
flow to the coronary arteries.
Blood flow to the brain [and the rest of the body] occurs when the heart
squeezes out blood during your chest compression.
THUS FOR GOOD BLOOD FLOW TO THE BRAIN AND THE HEART YOU
MUST DO A HARD CHEST COMPRESSION AND THEN ALLOW RECOIL.](https://image.slidesharecdn.com/ctexpo-150601173921-lva1-app6892/85/CT-EMS-EXPO-SCA-SYSTEMS-49-320.jpg)
![• There is a lot of data that hyperventilation is harmful in cardiac
arrests. There is a lot of data that any interruption in chest
compressions is harmful. If intubation will be done , it must not
interrupt chest compressions and ventilation cannot be
allowed to be too frequent [the AHA recommends 6-8 per
minute] .](https://image.slidesharecdn.com/ctexpo-150601173921-lva1-app6892/85/CT-EMS-EXPO-SCA-SYSTEMS-52-320.jpg)







![MA State Law on Dispatch
The 911 service must have a Medical director.
The service must do Quality Assurance [Q/A ] on
its calls, and
it must offer dispatch CPR over the phone to callers.
I will offer some ideas on Q/A .
The state of Massachusetts follows the guidelines of the American
Heart Association [AHA ] . The AHA offers clear guidance on
Dispatch CPR. I will present their policy.](https://image.slidesharecdn.com/ctexpo-150601173921-lva1-app6892/85/CT-EMS-EXPO-SCA-SYSTEMS-71-320.jpg)

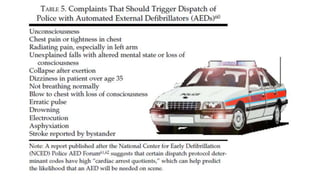
![AHA AND DISPATCH CPR
“ In nearly half of all cases in which
dispatchers provide CPR …instructions ,
the patient will not be in arrest. Serious
injury from bystander CPR is uncommon
[1-2%], but failure to provide bystander
CPR to people in cardiac arrest can be
lethal…](https://image.slidesharecdn.com/ctexpo-150601173921-lva1-app6892/85/CT-EMS-EXPO-SCA-SYSTEMS-74-320.jpg)
![Review the following data for every Run
• Was the arrest recognized ?
• Were the 2 Key Questions asked?
• Were agonal respirations recognized [if present]?
• Was cardiac arrest recognized in under 1 minute?
• Were telephone CPR instructions offered, and accepted by the
bystander? Do not ask if the bystander is willing, instruct them
what to do, people are more likely to follow your instructions
when told what to do than when offered options.](https://image.slidesharecdn.com/ctexpo-150601173921-lva1-app6892/85/CT-EMS-EXPO-SCA-SYSTEMS-84-320.jpg)













![The Key
• Push hard [to 2 inches]
• Push Fast [100 per minute]
• Recoil [get your hands off]
• And
• Don’t Stop [for 2 minutes]](https://image.slidesharecdn.com/ctexpo-150601173921-lva1-app6892/85/CT-EMS-EXPO-SCA-SYSTEMS-117-320.jpg)
![The Key on Rate
• The previous slide , from an ICU in Chicago , reveals 2 things , one is
that ROSC [return of circulation, and therefore survival ] is directly
related to the rate. The ROSC at a rate of 60 compressions per
minute is only ¼ as high as the rate of ROSC at 100 compressions
per minute.
• The other very important bit of data is that when the compression
rate exceeds 120 the rate of ROSC declines. You must maintain a
rate of 100.
• USE A METRONOME!!!!](https://image.slidesharecdn.com/ctexpo-150601173921-lva1-app6892/85/CT-EMS-EXPO-SCA-SYSTEMS-119-320.jpg)

![• There is a lot of data that hyperventilation is harmful in cardiac
arrests. There is a lot of data that any interruption in chest
compressions is harmful. If intubation will be done , it must not
interrupt chest compressions and ventilation cannot be
allowed to be too frequent [the AHA recommends 6-8 per
minute, the tidal volume should be 6 ml per Kg] .](https://image.slidesharecdn.com/ctexpo-150601173921-lva1-app6892/85/CT-EMS-EXPO-SCA-SYSTEMS-125-320.jpg)














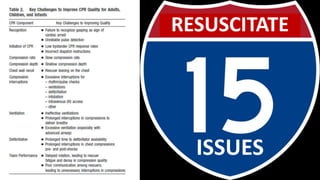
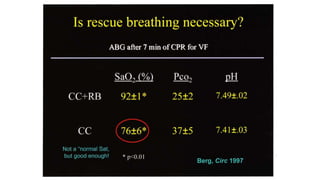
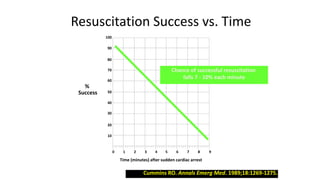
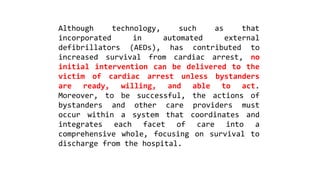
This document discusses improving cardiac resuscitation systems of care. It describes how some systems achieve survival rates over 50% for cardiac arrests due to ventricular fibrillation through coordinated efforts including bystander CPR, public access defibrillators, EMS response times, and post-resuscitation care. The document outlines key components of model systems including establishing registries to measure performance, improving layperson and EMS involvement in CPR, and decreasing time to access emergency care. It emphasizes that the overall system of care, not individual components, determines survival rates.























































































