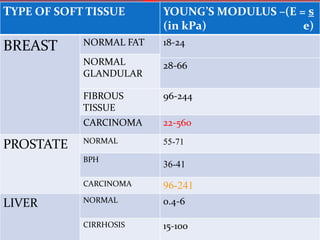
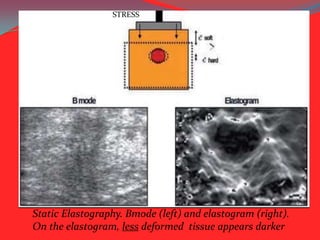
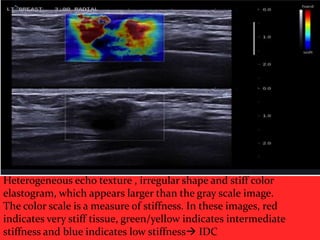
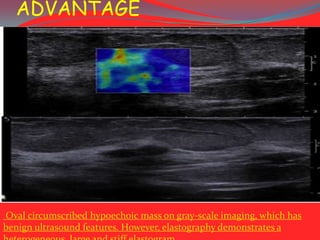
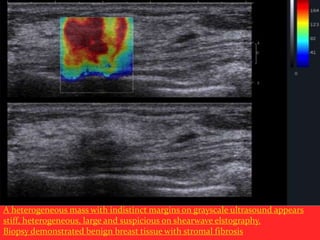
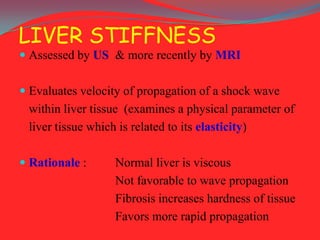
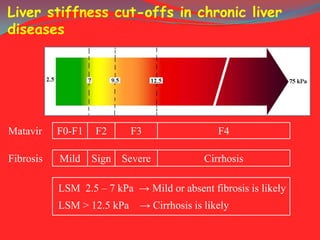
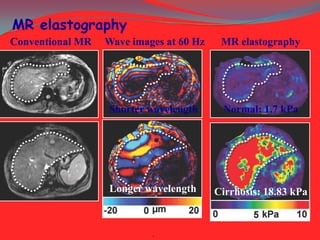
Elastography is a noninvasive imaging technique that uses ultrasound to image the elasticity or stiffness of tissues. It works by applying slight pressure and measuring how tissues deform. Hard tissues appear stiffer on elastograms. Elastography has many medical applications including differentiating benign from malignant breast lesions, assessing liver fibrosis, and evaluating prostate lesions. Shear wave elastography provides quantitative stiffness measurements and is the most accurate method. While useful, elastography has limitations such as difficulty imaging large or painful lesions and certain anatomical areas. Overall, elastography provides important clinical information about tissue composition when used along with other imaging tests.



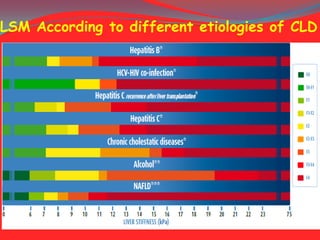

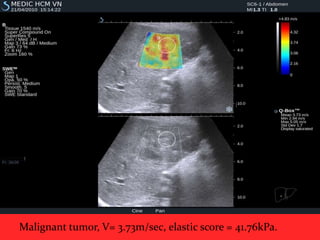
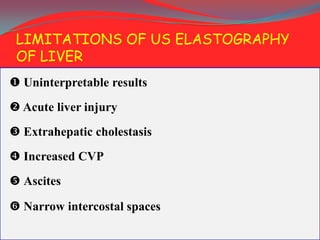
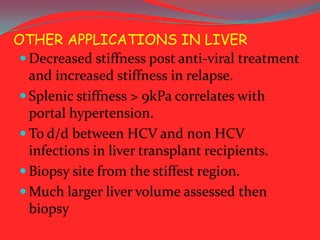









































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)














