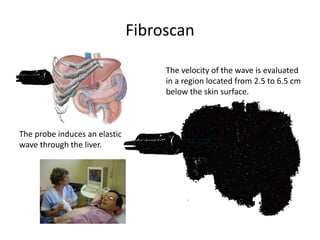
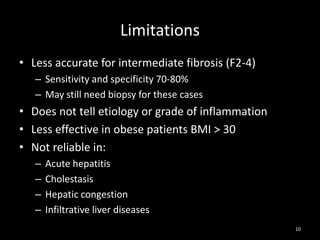
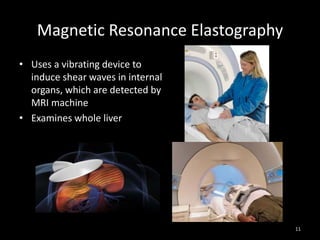

The document discusses methods for detecting early liver fibrosis, emphasizing the importance of measuring fibrosis for prognosis and treatment decisions. It compares traditional liver biopsy with non-invasive techniques like ultrasound, Fibroscan, and magnetic resonance elastography, highlighting their benefits and limitations. Fibroscan is noted for being a painless and accurate tool for detecting early fibrosis, although it may not be suitable for individuals with obesity or certain liver conditions.























![[2016] pathogenesis of liver fibrosis](https://cdn.slidesharecdn.com/ss_thumbnails/2016pathogenesisofliverfibrosis-160113191600-thumbnail.jpg?width=640&height=640&fit=bounds)









































































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)








