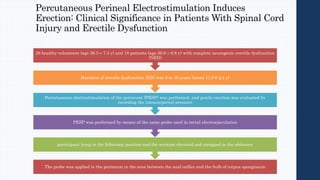
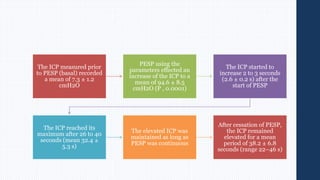
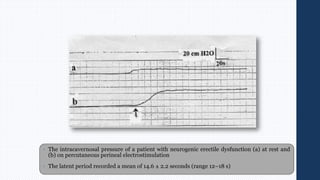
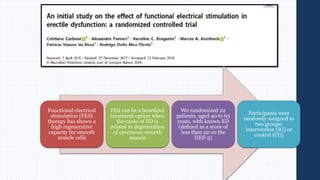
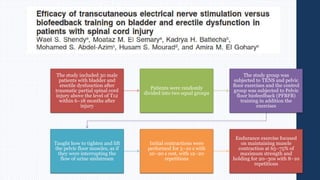
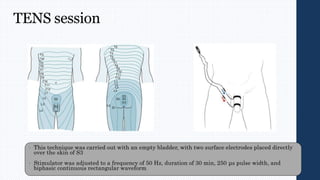
Electrical stimulation of the perineum can induce erection in men with erectile dysfunction. A study stimulated the perineum of 18 men with complete neurogenic erectile dysfunction and measured intracavernosal pressure, finding it increased significantly from 7.3 cmH2O at baseline to 94.6 cmH2O during stimulation. Erection was maintained as long as stimulation continued. Functional electrical stimulation therapy has also shown benefits for smooth muscle regeneration in the penis. Another study found that men with bladder and erectile dysfunction after spinal cord injury experienced greater improvements in erectile function with a combination of pelvic floor exercises and transcutaneous electrical nerve stimulation compared to exercises alone.

![Pathologic processes in these regions, such as Parkinson’s disease, stroke, encephalitis, or temporal lobe
epilepsy, are often associated with ED
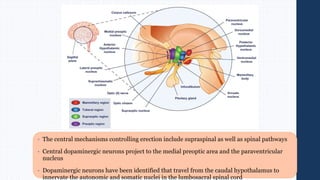
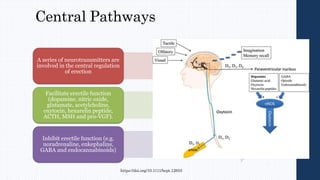
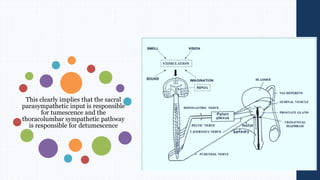
The MPOA, the paraventricular nucleus, and the hippocampus have been regarded as important
integration centers for sexual drive and penile erection
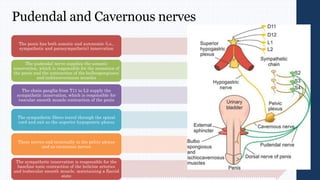
Because an erection is a neurovascular event, any disease or dysfunction affecting the brain, spinal cord,
cavernous and pudendal nerves can induce dysfunction
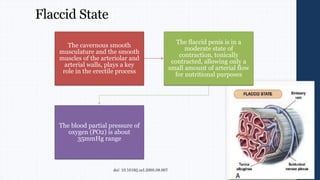
Some are based on the cause (diabetic, iatrogenic, traumatic) and some on the neurovascular mechanism of
the erectile process failure to initiate [neurogenic], failure to fill [arterial], and failure to store [venous]
Many classifications have been proposed for ED.
doi: 10.1016/j.ucl.2005.08.007](https://image.slidesharecdn.com/erectiledysfunction-220528155454-69360dab/85/erectile-dysfunction-pptx-4-320.jpg)









































![Erectile Dysfunction [Dr. Edmond Wong]](https://cdn.slidesharecdn.com/ss_thumbnails/ededmond-140716212750-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)




































![ONFH[AVN HIP] -TRIPLE REGIME -A NOVAL SURGICAL CONCEPT .pptx](https://cdn.slidesharecdn.com/ss_thumbnails/onfhavnhip2026koaconcalicutdrgokuldevdrmashraf-260210064517-213ec005-thumbnail.jpg?width=640&height=640&fit=bounds)













![CTEV [ clubfoot] DR ARUN LAL ,DR MOHAMED ASHRAF travancore medical college k...](https://cdn.slidesharecdn.com/ss_thumbnails/ctevclubfootdrarunlaldrmohamedashraftravancoremedicalcollegekollamkeralaindia-260208063247-18fc466c-thumbnail.jpg?width=640&height=640&fit=bounds)


