Downloaded 54 times
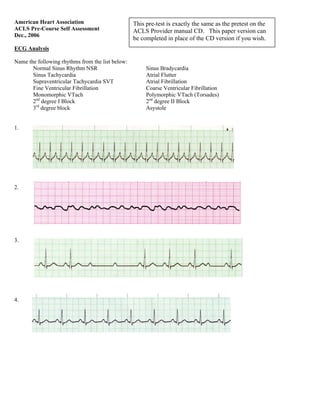












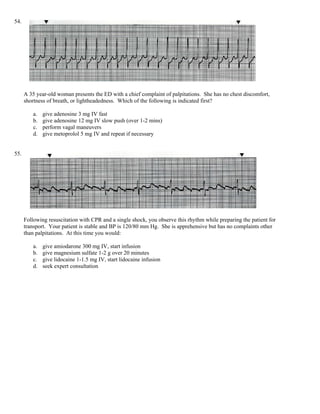






This document contains an ACLS pre-course self-assessment test covering ECG rhythm identification, pharmacology, and practical application questions. It is intended as a practice test to prepare for the ACLS provider course. The test contains multiple choice questions testing knowledge of cardiac arrest treatment algorithms, medications, and rhythms commonly assessed in ACLS.



































































