Downloaded 115 times

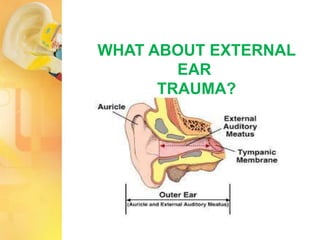
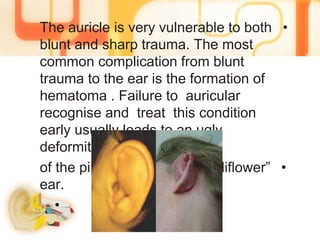
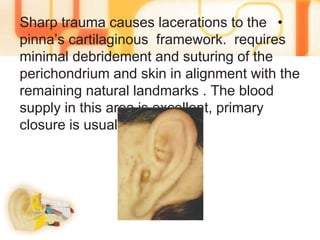
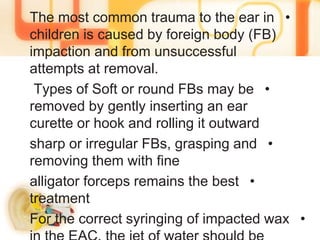
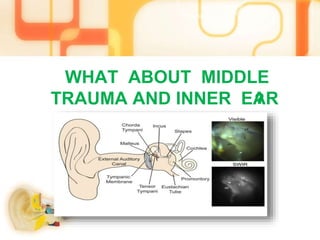


Ear trauma can occur from a variety of causes including loud noises, explosions, burns, and physical impacts. External ear trauma commonly results in bruising or lacerations to the auricle or pinna. Impacts can deform the ear over time into a "cauliflower" shape if not treated. Foreign objects in the ear should be removed carefully to avoid further injury. Thermal burns produce swelling and pain. Changes in pressure like from diving can rupture blood vessels in the middle ear. Head injuries sometimes fracture the skull and temporal bone, risking damage to the middle ear structures, hearing loss, and facial nerve involvement.























































































