Developmental Anatomy
DISEASES OF PINNA
1.Congenital Disorders
a. Anotia
b. Skin tags
c. Microtia
d. Macotia
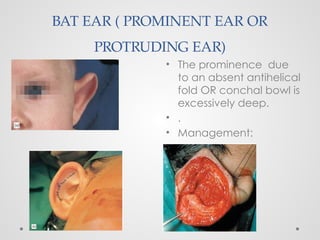
e. Bat ear
f. Collapsed ear
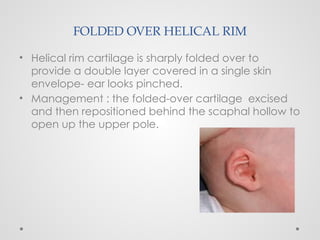
e. Folded over helical rim
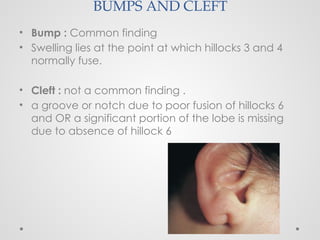
g. Bumps and cleft
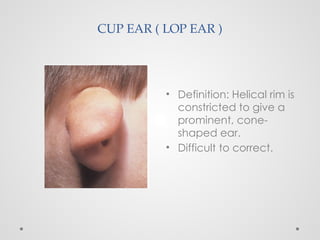
h. Cup ear
i. Crytotia
j. Positional problems
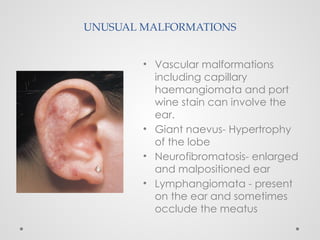
k. Unusual malformations
l. Stahl’s ear
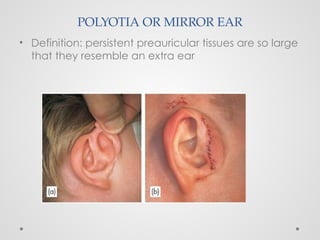
m. Polyotia
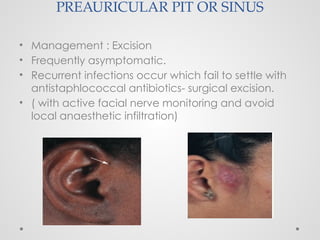
n. Preauricular pit
2.Trauma to auricle
a. Hematoma of the auricle
b. Frostbite
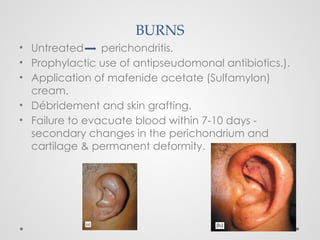
c. Burns
3. Inflammatory Disorders
a. Peicondritis
b. Relapsing Pericondritis
DISEASES OF EXTERNAL AUDITORY CANAL
1.Inflammatory Disorders
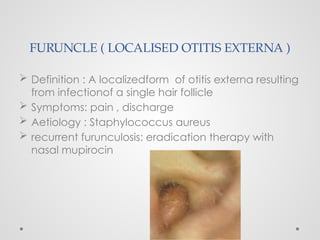
a. Furuncle
b. Diffuse Otitis Externa
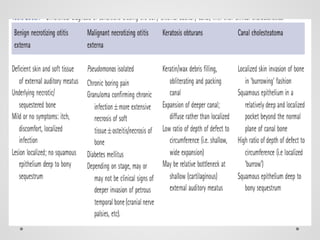
c. Benign Necrotizing Externa
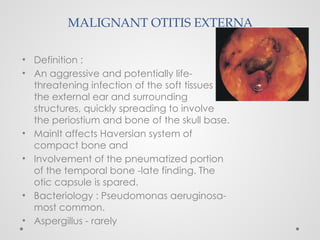
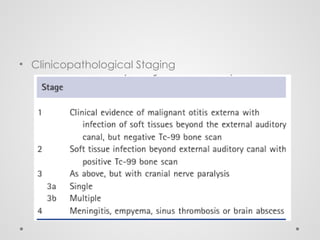
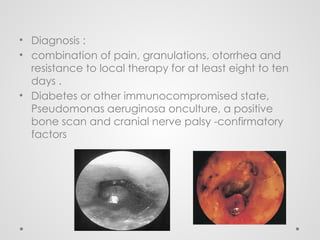
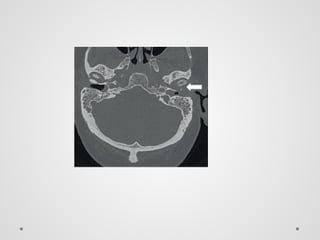
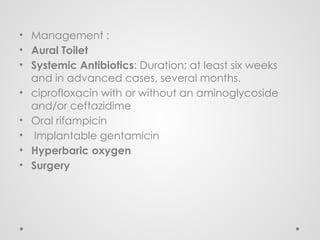
d. Malignant Otitis Externa
e. Herpes Zoster Oticus
f. Otomycosis
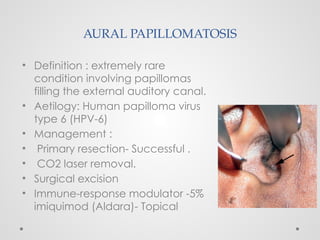
g. Aural Papillomatosis