Download to read offline
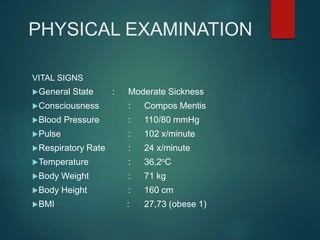
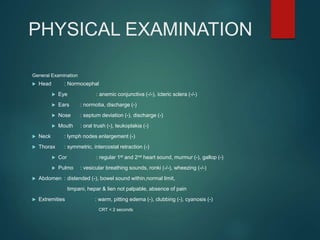
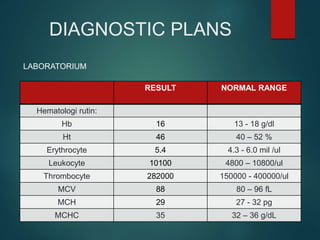
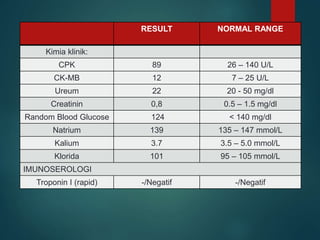
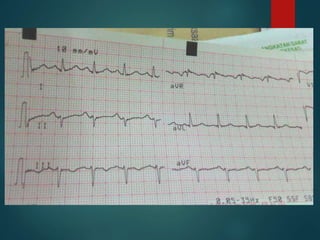
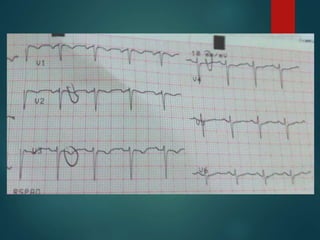
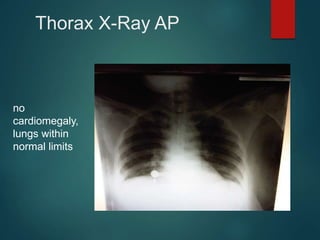
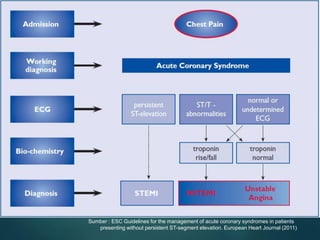
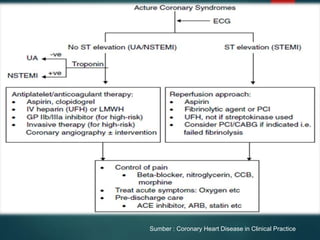
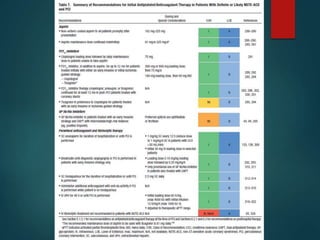

1. Mrs. L, a 41-year-old woman, presented to the emergency room with chest pain for 3 days. Physical examination found her heart rate was 102 beats per minute. 2. Tests including ECG, bloodwork, chest x-ray were largely normal. The ECG showed ST depression. 3. She was assessed with unstable angina pectoris and prescribed aspirin, clopidogrel, nitroglycerin, and bisoprolol to treat her symptoms. Her prognosis was noted to be uncertain.