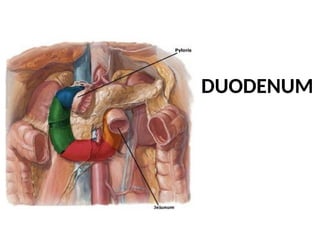
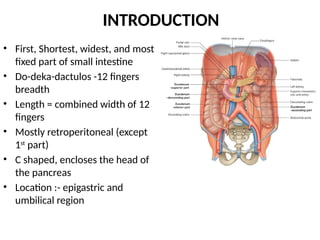
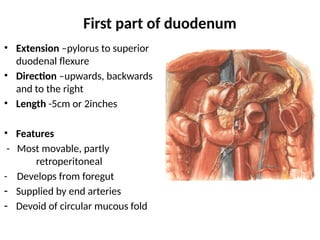
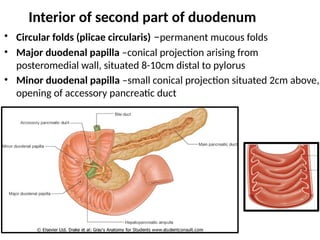
The duodenum is the first and shortest section of the small intestine, divided into four parts with specific lengths and relations to surrounding organs. It plays a critical role in digestion and is prone to certain medical conditions such as peptic ulcers. Its structure includes serosa, muscularis externa, submucosa, and mucosa, with detailed blood supply and nerve innervation described in the document.