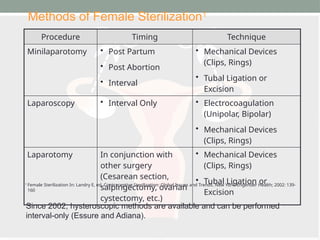
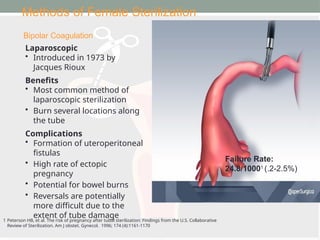
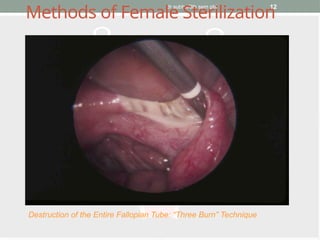
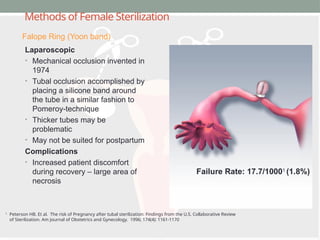
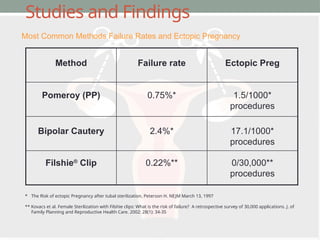
The document provides an overview of female sterilization methods, highlighting the historical context, various techniques employed, and their associated failure rates. It discusses the demographics of women opting for these procedures, as well as considerations and potential regrets following sterilization. The findings emphasize the importance of informed consent and the permanent nature of these methods.