
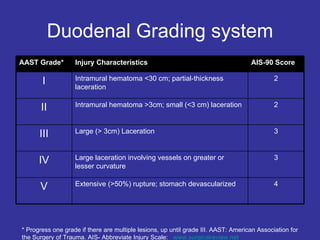
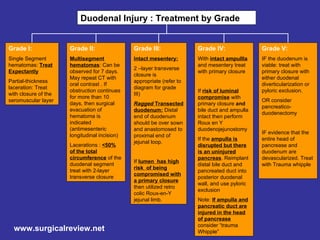

1. The document presents a treatment algorithm for grading duodenal injuries from Grade I to Grade V based on the severity of the injury. 2. Mild injuries like hematomas or partial-thickness lacerations are often observed or treated with closure. More severe injuries may require primary closure, resection, or bypass procedures like Roux-en-Y reconstruction. 3. For Grade III injuries, 2-layer closure is appropriate if the mesentery is intact, while more severe injuries may require resection and anastomosis or bypass depending on the extent of injury to surrounding structures.























































































