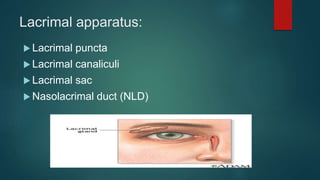
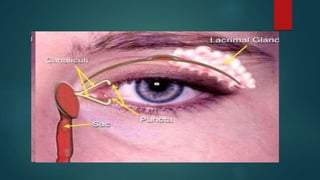
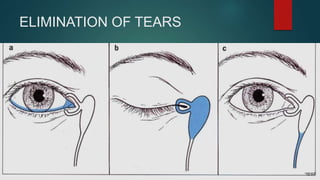
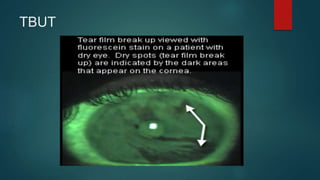
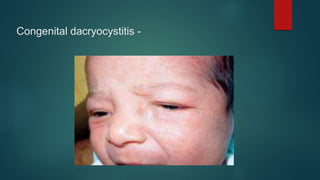
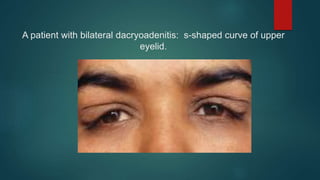
The document discusses the anatomy and physiology of the lacrimal system and tear film. It describes the main structures of the lacrimal apparatus including the lacrimal gland, accessory lacrimal glands, lacrimal passages, puncta, canaliculi, lacrimal sac, and nasolacrimal duct. It discusses tear film layers, secretion, and functions. It also summarizes common lacrimal system disorders like dry eye, dacryocystitis, epiphora, dacryoadenitis and their signs, symptoms, etiologies, and treatments. Surgical procedures for these conditions like dacryocystorhinostomy are also briefly outlined.