Download to read offline


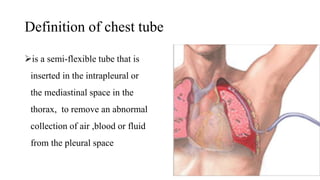
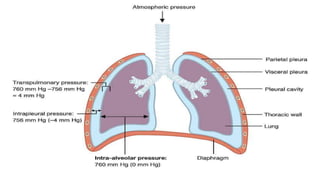
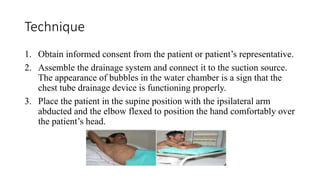
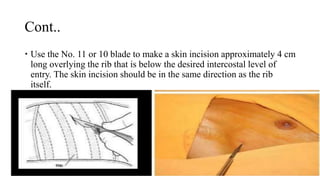
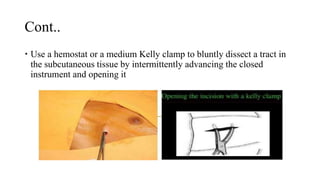

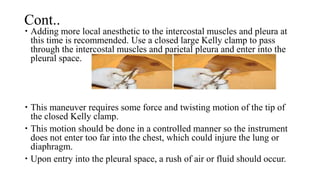


The document discusses chest tubes, which are tubes inserted into the pleural space or mediastinum to drain fluid, air, or blood. It describes the anatomy of the pleural space and lungs, indications for chest tubes including pneumothorax and fluid drainage, proper chest tube insertion technique, drainage systems, complications, and removal criteria.