Downloaded 227 times



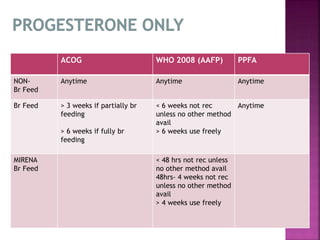

Contraception in the postpartum period differs due to breastfeeding, increased risk of blood clots, and unpredictable ovulation. Counseling should occur during antenatal and postnatal periods. Options include breastfeeding, progestin-only pills, implants, IUDs, sterilization, condoms. Timing of use depends on breastfeeding status and bleeding risk. Recommendations balance effectiveness, safety, and ease of use while supporting breastfeeding.























































































