FP and itsfocus on IUCD, Postpartum FP and counselling
skills an overview
Mr.Rudrappa Angadi(MPH)
Program officer EAISI project
Jhpiego-Chhattisgarh
2.
Course Goals
• Toinfluence in a positive way the attitudes of
the students toward the concepts of Family
Planning (FP).
• To provide updated knowledge on IUCD, Post
partum FP and counselling skills.
3.
Learning Objectives
• Toknow the meaning of FP
• Unmet need
• Overview of IUCD
• Medical Eligibility Criteria
• Post-partum FP
• Counselling
4.
FP in RMNCH+AStrategy
• Family planning means that the couples decide and plan when and how
many children they want to have
• Family planning is central to improve maternal and newborn survival and
health, not just for population stabilization
• Family planning can avert
> 30% of maternal deaths
>10% of child mortality
• FP save women’s lives and health by preventing unwanted, closely spaced
and mistimed pregnancies and thus avoiding pregnancies with higher risks
and chances of abortions, many of which may be unsafe.
5.
Unmet need forFamily Planning
WHO Definition:
• Women with unmet need are those who are fecund
and sexually active but are not using any method of
contraception, and report not wanting any more
children or wanting to delay the next child.
• Women in reproductive age group, who want to
avoid or delay pregnancy but are not using any form
of family planning.
6.
Unmet Need forFamily Planning in India
As per DLHS 3 (2007-08)
Unmet need for family planning is 20.5%
- 7.2% unmet need for spacing (delaying next pregnancy)
- 13.3% unmet need for limiting (avoiding any further
pregnancy)
Unmet need and Non Users ????????????
7.
Overview of CopperIUCD
A small, flexible polyethylene impregnated with barium
sulfate frame containing copper
2 types of Cu IUCDs available under the national program
1. Cu IUCD 380A
2. Cu IUCD 375
8.
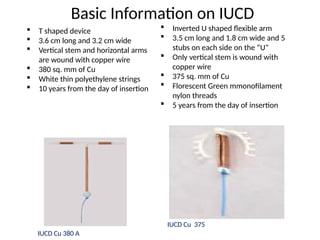
Basic Information onIUCD
T shaped device
3.6 cm long and 3.2 cm wide
Vertical stem and horizontal arms
are wound with copper wire
380 sq. mm of Cu
White thin polyethylene strings
10 years from the day of insertion
Inverted U shaped flexible arm
3.5 cm long and 1.8 cm wide and 5
stubs on each side on the “U”
Only vertical stem is wound with
copper wire
375 sq. mm of Cu
Florescent Green mmonofilament
nylon threads
5 years from the day of insertion
IUCD Cu 380 A
IUCD Cu 375
9.
Global use ofIUCD
Recent estimates suggest that almost one in five married contraceptive users is
currently using an IUCD
10.
IUCD Usage inIndia
Source: DLHS -3 (2007-2008), IIPS, Mumbai
IUCD is one of the most effective reversible and safe contraceptive methods, but still
remains largely underutilized.
11.
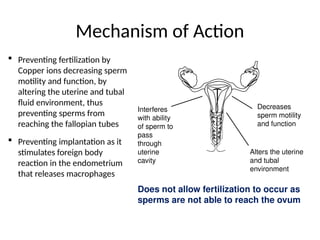
Mechanism of Action
Preventing fertilization by
Copper ions decreasing sperm
motility and function, by
altering the uterine and tubal
fluid environment, thus
preventing sperms from
reaching the fallopian tubes
Preventing implantation as it
stimulates foreign body
reaction in the endometrium
that releases macrophages
Decreases
sperm motility
and function
Interferes
with ability
of sperm to
pass
through
uterine
cavity
Alters the uterine
and tubal
environment
Does not allow fertilization to occur as
sperms are not able to reach the ovum
12.
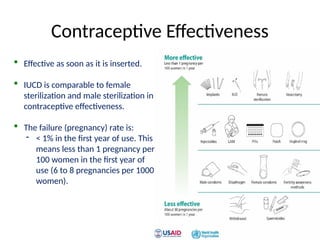
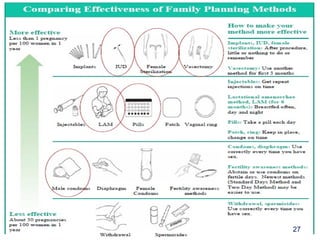
Contraceptive Effectiveness
Effectiveas soon as it is inserted.
IUCD is comparable to female
sterilization and male sterilization in
contraceptive effectiveness.
The failure (pregnancy) rate is:
- < 1% in the first year of use. This
means less than 1 pregnancy per
100 women in the first year of
use (6 to 8 pregnancies per 1000
women).
13.
Advantages of CuIUCD
Offers long-term, highly effective reversible protection against pregnancy.
Effective and Reversible.
Suitable for use by most women.
Can be used as an emergency contraceptive .
It can be replaced, without any gap, and be used as an alternative to terminal method.
Does need special attention.
Insertion is one time and simple procedure and is cost effective.
Can be used by lactating women.
Does not interact with any medicines the client may be taking.
Easily accessible and affordable
14.
Limitations of CuIUCD
Requires skilled provider .
Pelvic examination is necessary before insertion.
Does not protect against STIs/ HIV.
Cannot be inserted in women with active RTI/STI.
Cannot be inserted in women who currently have PID.
15.
Side Effects ofIUCDs
Unpleasant but are not harmful and usually subside or resolve
within a few months after insertion.
Menstrual changes:
- Increase in the duration/amount of menstrual bleeding
- Spotting or light bleeding during the first few days or months
after insertion.
Discomfort or cramps during insertion and for the next few days
which subsides in due course.
16.
Possible Complications
Potential healthrisks which are uncommon or rare, are:
Spontaneous expulsion occurs in about 2-8 % clients.
(most likely to occur during the first three months after insertion, and during
menstrual periods).
If pregnancy occurs with the IUCD in situ, there is a risk of spontaneous abortion,
sepsis and ectopic pregnancy; no adverse effects on the fetus.
Infection following insertion is less than 1% -risk is highest during the first 20 days
after insertion. Due to non compliance to IP practices, rather than the device itself.
Uterine perforation during insertion is a rare complication which occurs in 0.5 - 1.5
per 1000 insertions and is associated with the level of provider's skill and
experience.
Objectives
By the endof this session the Students will be able to:
• Discuss methods of Postpartum Family Planning
• Describe the specific situations of postpartum women
• Discuss breastfeeding and LAM
• List opportunities and mechanisms for post partum FP
integration
19
20.
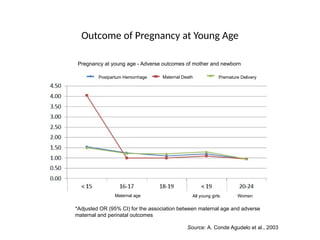
Outcome of Pregnancyat Young Age
Postpartum Hemorrhage Maternal Death Premature Delivery
Maternal age All young girls Women
Source: A. Conde Agudelo et al., 2003
*Adjusted OR (95% CI) for the association between maternal age and adverse
maternal and perinatal outcomes
Pregnancy at young age - Adverse outcomes of mother and newborn
21.
The Postpartum Period
Post-placentalperiod
The first 10 minutes after placenta delivery .
Immediate postpartum
Up to 48 hours after giving birth.
Early postpartum
48 hours to 6 weeks after giving birth.
Extended postpartum
6 weeks to 1 year after giving birth.
22.
Definitions
Birth to pregnancyinterval:
Time period between a live birth and the start of the next
pregnancy
Birth to birth interval:
Time period between a live birth and the next live birth
23.
WHO Technical Recommendationson Pregnancy
Spacing
Recommendation for spacing after a live birth:
o The recommended interval before attempting the next pregnancy is
at least 24 months
o The recommended interval between two live births is at least 36
months
Recommendation for spacing after abortion:
o The recommended interval for the next pregnancy should be at least
6 months
24.
Outcomes of Motherand New born of
short birth interval
Short birth to pregnancy (BTP) intervals <24 months are
associated with increased risk of:
For Mother
Maternal death
Induced abortion
Miscarriage
Premature Labor
Antepartum/Postpartum
Hemorrhage
Anemia
For New born
Low birth weight baby
Premature baby
Neonatal death
25.
Post Abortion Outcomes
Intervalbetween post abortion and next pregnancy, if less than 6
months, the following risks increases:
Premature rupture of membrane
Maternal anemia
Premature delivery
Low for birth weight baby
IUGR
26.
Return to Fertilityafter Delivery or Abortion
• 5-10% of breastfeeding women get pregnant in first year postpartum
• Fertility returns before menses
• Contraceptive methods…..??????? and effectiveness…??????????????
Condition of woman Return to fertility
Breastfeeding
- Using LAM accurately (All 3
criteria fulfilled for 6 months)
− Sometime after 6 months -
variable
- Breastfeeding without using LAM − Possibly even before 6 months,
but again, variable
− Average is 45 days
Non-Breastfeeding − 3 weeks or 21 days postpartum
After abortion − 2 weeks or 10-14 days post-
abortion
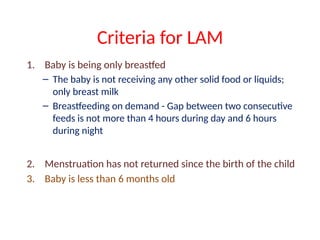
Criteria for LAM
1.Baby is being only breastfed
– The baby is not receiving any other solid food or liquids;
only breast milk
– Breastfeeding on demand - Gap between two consecutive
feeds is not more than 4 hours during day and 6 hours
during night
2. Menstruation has not returned since the birth of the child
3. Baby is less than 6 months old
31.
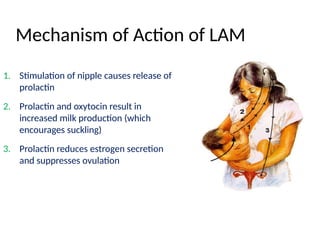
Mechanism of Actionof LAM
1. Stimulation of nipple causes release of
prolactin
2. Prolactin and oxytocin result in
increased milk production (which
encourages suckling)
3. Prolactin reduces estrogen secretion
and suppresses ovulation
32.
Effectiveness of LAM
•LAM is 99.5% effective with consistent and correct use;
and more than 98% effective as typically used
• Effectiveness is same as other effective modern
methods
33.
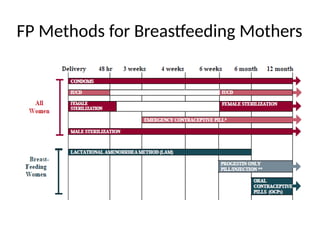
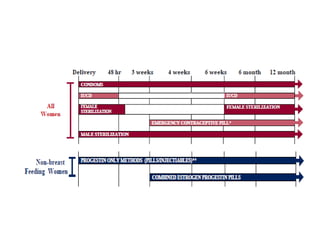
Timings of integrationof PPFP Services With Other
Services
ANC
Immediately after delivery
Postpartum check up for mother or baby
At the time of discharge from hospital
Contacts for mother/baby check up during 1-6 weeks postpartum
Immunization visits
After delivery, make postpartum family planning services
available to women/ couples as per their need
Counselling is atype of client – provider interaction that
involves two – way communication between a health care staff
member and a client for the purpose of confirming or facilitating
an informed decision by the client or helping the client address
problems or concerns.
36.
Counselling
The purpose offamily planning counseling is to help women
and couples to choose family planning method according to
their choice to prevent unwanted pregnancy.
Counseling will help client to:
Choose the best option for them from available contraceptive
methods
Correctly use the chosen method
Continue use of chosen method
37.
Clients who startmethod of their choice after complete
information are satisfied clients and then the possibility of
continuation of the method is high.
Types in FPcounselling
General counselling
Method specific counselling
Follow-up counselling
41.
Family Planning Counseling…
GeneralCounseling
If the couple has already decided to have the next baby after few
years and not early, then
Tell them - to prevent unwanted pregnancy and for good
health of mother and baby, they should use any contraceptive
method for at least 2 years after childbirth
Ask - If have they have thought of using any contraceptive
method after delivery? If yes, then what do they know about
the method.
41
42.
Family Planning Counseling…
GeneralCounseling…
Help client to choose method of choice after basic
information on all methods
Give information on PPFP methods and PPIUCD
Clarify, if they have any mistaken beliefs or misconceptions
about specific family planning methods
On the basis of key information, help woman or couple to
choose method of their choice
42
43.
Family Planning Counseling…
Methodspecific counseling
Give detailed information of the chosen method like:
How does the method act
How effective the method is
What are its benefits
Does it affect breastfeeding or not
Does it protect from sexually transmitted infections
Common side effects of the method and their treatment
When to come for follow-up
43
44.
How to doFollow-up of
Family Planning Clients
Follow-up counseling
Greet client and ask the purpose of visit
Encourage to continue the method if client has no concerns or problems
Repeat if client has forgotten any important information
Reassure client about side effects that these will be resolved on their own
within a few months
If client wants to change the method, help her/couple to choose another
method
44
45.
New client witha method in mind
Ensure that client knows about other options
o This can be done through group discussion
Check that the client has correct information about
her chosen method
Support client if she is medically eligible for the
method
Discuss with client about method’s use and
management of side effects
46.
References
• http://www.fhi.org/training/en/modules/AFTER/default.htm (accessedApril 14, 2010).
• Ross, J.A. and W.L. Winfrey. 2001. “Contraceptive use, intention to use and unmet needs during
• the extended postpartum period.” International Family Planning Perspectives 27, no. 1: 20-7.
• Speroff, L. and D.R. Mishell Jr. 2008. “The postpartum visit: It’s time for a change in order to
• optimally initiate contraception.” Contraception 78, no. 2: 90-98.
• United Nations Population Fund. 2004. State of the world population 2004.
• http://www.unfpa.org/swp/2004/english/ch9/page5.htm (accessed February 15, 2010).
• World Health Organization/Department of Reproductive Health and Research (WHO/RHR) and
• Johns Hopkins Bloomberg School of Public Health/Center for Communications Programs (CCP),
• Knowledge for Health Project. Family Planning: A global handbook for providers (2008 update).
• Baltimore and Geneva: CCP and WHO/RHR.
47.
Talk to yourselfat least once in a Day.. Otherwise you
may miss a meeting with an EXCELLENT person in this
World………..
-Swami Vivekananda
Thank You for your Kind attention
Editor's Notes
#20 *There is another aspect around helping women achieve healthy pregnancy outcomes in addition to improved spacing, and this is related to the timing of pregnancy.
* Here you see the relationship between “early maternal age and adverse outcomes.”
* Controlling for all other factors, compared to women aged 20-24, a 16-17 year old adolescent is approximately 1.25 times more likely to hemorrhage or experience very preterm delivery.
*But look at the <15 group. Data shows that an adolescent under 15 years old is four times more likely to die giving birth, and 1.5 times more likely to hemorrhage or experience very preterm delivery compared to a pregnant woman aged 20-24.
#31 LAM prevents pregnancy by interfering with the release of hormones that allow ovulation.
Suckling stimulates production of a hormone that tells the brain/hypothalamus not to release the hormone necessary for ovulation. Regular and frequent nipple stimulation is necessary to ensure a continuous stimulation of the brain/hypothalamus.
With weaning, prolactin levels decline and with cessation of breastfeeding ovulation resumes within 14–30 days.
Please look in your reference manual for a more detailed description of this mechanism of action.
#32 What do we mean by “consistent and correct” and “typically used”? “Consistent and correct use” is the best rate a user can expect from this method. “Typical use” is the average rate of protection. Some will be more successful and some will be less successful than this.
LAM is more than 98% effective with typical use. How do you think this compares with combined oral contraceptives? [Allow answer from participants] COCs are only 92% effective with typical use.
LAM effectiveness reference: World Health Organization (WHO/RHR) and Johns Hopkins Bloomberg School of Public Health/Center for Communications Programs (CCP), INFO Project. Family Planning: A Global Handbook for Providers. Baltimore and Geneva: CCP and WHO, 2007.