Case- 1
19yr old unmarried presents to discuss regarding
contraception
No significant medical history,
Does not take any medications regularly
Sexually active with male partners
How are u going to approach her?
What contraceptive do you recommend?
6.
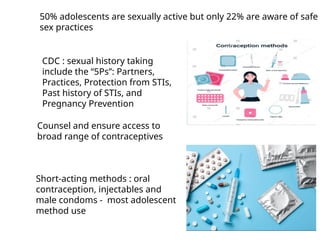
50% adolescents aresexually active but only 22% are aware of safe
sex practices
Counsel and ensure access to
broad range of contraceptives
Short-acting methods : oral
contraception, injectables and
male condoms - most adolescent
method use
CDC : sexual history taking
include the “5Ps”: Partners,
Practices, Protection from STIs,
Past history of STIs, and
Pregnancy Prevention
7.
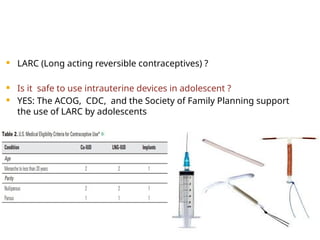
LARC (Longacting reversible contraceptives) ?
Is it safe to use intrauterine devices in adolescent ?
YES: The ACOG, CDC, and the Society of Family Planning support
the use of LARC by adolescents
8.
Is there anycomplication with IUD use ?
PID
STI
Future infertility
Uterine perforation
Difficult insertion
Intrauterine Device Expulsion
AUB
9.
The riskof PID with IUD placement is 0–
2% when no cervical infection is present
0–5% when insertion occurs with an
undetected infection
With long-term use, levonorgestrel IUDs
may lower the subsequent risk of PID by
thickening cervical mucus and thinning
the endometrium
10.
STI Screening?
CDC: Should be screened for gonorrhea and chlamydial infection at
the time of IUD insertion
Appropriate to screen for STIs and place an IUD on the same day.
Routine antibiotics?
Routine antibiotic prophylaxis is not recommended at the time of IUD
insertion
If an STI is diagnosed after the IUD is in place, it may be treated
without removing the IUD
Dual method should be practised to avoid STD
11.
The riskof uterine perforation for adolescents -
approximately 0.1%
IUD expulsion rates range from 2% to 10% for all IUD
users
Do Intrauterine Devices Increase an Adolescent’s Risk of
Infertility ?
Infertility is not more likely to occur after IUD
discontinuation than after discontinuation of other
reversible methods of contraception
Baseline fecundity returns rapidly after IUD removal
12.
Is it difficultinsert Intrauterine Devices in Adolescents and
Nulliparous Women?
Not been shown to be more difficult in adolescent or in
nulliparous patients compared with parous women.
In a cohort of 1,177 adolescents and women aged 13–24
years, successful IUD placement was achieved on first
attempt in 96% of patients.
Provision of additional analgesia during IUD insertion
should be individualized and may include NSAIDs,
narcotics, anxiolytics, or paracervical blocks.
Misoprostol should not be routinely used before IUD
insertion
13.
The Contraceptive Implant
Has minimal or no effect on bone density or weight
Changes in bleeding patterns is the most common
reason for implant discontinuation
14.
NACO: ABCapproach in promoting safe
sex practices among adolescents
A- Abstinence, delay the first sexual
activity
B- Being faithful, involving with single
partner in a monogamous relationship
C- Condom, correct and complete use to
protect against HIV, STI, unwanted
pregnancy
15.
Patient decideson Depo Provera
What about bone density?
WHO(2005) : No restriction on the use of
DMPA in women aged 18–45 years, including
no restriction on the duration of use.
Case 2
A26yr old married for 5 months wants to
postpone her pregnancy for 1-2yr
Presently using condoms but she wants more
reliable method
Frequent traveller and used to have irregular
cycles sometimes with heavy flow
What additional information do you want
Which contraception will you suggest?
18.
Details ofM/H
Assessment of medical eligibility
Assessment of medical history & life style factors
Hypertension ? or VTE ?
H/O of migraines with aura
A drug history
Family H/o thrombotic disorder
General & Pelvic examination
Her BMI is 24kg/m2. She has mild asthma not on any
medication and has family h/o of HTN
19.
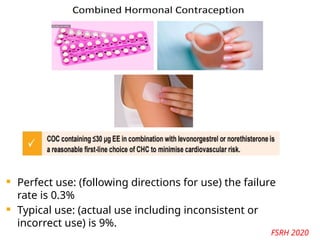
Perfect use:(following directions for use) the failure
rate is 0.3%
Typical use: (actual use including inconsistent or
incorrect use) is 9%.
FSRH 2020
20.
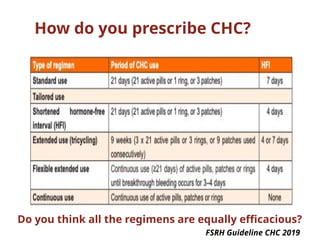
How do youprescribe CHC?
Do you think all the regimens are equally efficacious?
FSRH Guideline CHC 2019
21.
What are theadvantage of this tailored
regimen?
Reduced frequency of menses
Control HMB & dysmenorrhoea
Decrease in frequency of withdrawal
bleeds and associated symptoms (e.g.
headache, mood change) is reduced
22.
If she isobese or overweight?
Intrauterine IUD/IUS and ENG implant
recommended first line if BMI >25
Combined Hormonal contraception
MEC 2 if BMI 30-34
MEC 3 if BMI >34
23.
Case 3
26 yrNulligravida desires contraception
Not planning childbearing in near future
Currently using condoms
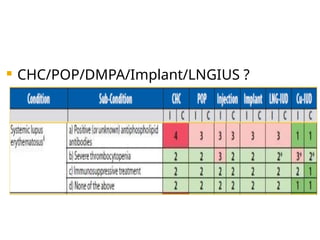
P/H: SLE, anemia, dysmenorrhea,PE, sickle trait
Meds: HCQ ,immunosupressant, prednisolone,
lisinopril, atorvastatin, omeprazole
What contraceptive would you recommend?
Case 4
30yr Primigravida at 36 weeks
gestation seen for routine prenatal care
Would like to discuss postpartum
contraception
Plans to breastfeed
Desires future fertility
What are your recommendations?
IMPLANON (etonogestrel implant)is a progestin-only, soft, flexible implant
preloaded in a sterile, disposable applicator for subdermal use. The implant is
off-white, non-biodegradable and 4 cm in length with a diameter of 2 mm (see
Figure 22). Each implant consists of an ethylene vinylacetate (EVA) copolymer
core, containing 68 mg of the synthetic progestin etonogestrel, surrounded by
an EVA copolymer skin. Once inserted subdermally, the release rate is 60 to 70
mcg/day in Week 5 to 6 and decreases to approximately 35 to 45 mcg/day at
the end of the first year, to approximately 30 to 40 mcg/day at the end of the
second year, and then to approximately 25 to 30 mcg/day at the end of the third
year.IMPLANON is a progestin-only contraceptive and does not contain
estrogen. IMPLANON does not contain latex and is not radio-opaque.
31.
Case 5
23yr married 3months ago comes in to
get emergency contraception. She had
unprotected intercourse last night.
Her LMP started 12 days ago
she has a regular monthly cycle.
She doesn’t take any medications.
Her BMI is 32kg/m2
What if she presents 4 days later?
How do you follow her up?
No restrictionsfor the medical eligibility of who can use ECPs
ECPs were found to be less effective in obese women (BMI> 30 kg/m2)
Should not be used repeatedly
do not harm future fertility
no delay in the return to fertility
MEC category 3 or 4 (with current PID, puerperal sepsis, unexplained vaginal bleeding, cervical
cancer, or severe thrombocytopenia) should not use a copper IUD as EC
IUCD can be inserted upto 4 days after ovulation i.e. day 19
in 28 days cycle
FOLLOWUP:
3-4weeks after or anytime in between in case of abdominal
pain/bleeding P/V
34.
Case 6
43-year-old womanpresented with
complaints of heavy and irregular menstrual
periods
10 kg weight gain in the past year, and acne
She was not using any contraceptive
method.
Biopsy revealed a disordered proliferative
endometrium
35.
Which methodsof contraception are
safe and suitable for her
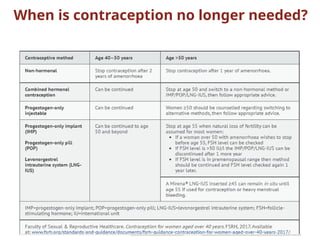
When contraception should be stopped
If she wants MHT ?
36.
Counselling ?
Naturaldecline in fertility with age
Should be counselled about effective contraception until
menopause or age 55 years, whichever occurs first
She needs contraception with non-contraceptive benefits
Age-related increased background risk of cardiovascular
disease, obesity and of breast and most gynaecological
cancers which may affect choice of contraceptive
method.
37.
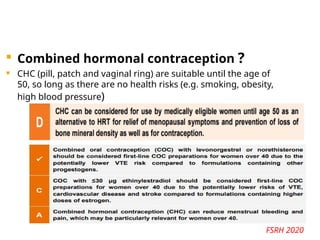
Combined hormonalcontraception ?
CHC (pill, patch and vaginal ring) are suitable until the age of
50, so long as there are no health risks (e.g. smoking, obesity,
high blood pressure)
FSRH 2020
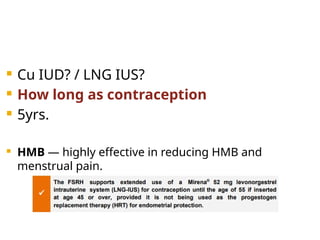
Cu IUD?/ LNG IUS?
How long as contraception
5yrs.
HMB — highly effective in reducing HMB and
menstrual pain.
40.
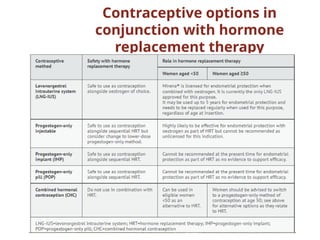
Progestogen-only implant ?
No age restriction and it can be used safely until a
woman no longer requires contraception, licensed
for 3 years and extended use is not supported,
regardless of age.
Not licensed for use as endometrial protection
and should not be used as the progestogen
component of HRT
41.
Progestogen-only injectable contraceptives?
DMPA is not licensed for use as endometrial
protection with oestrogen replacement and should
not be used as the progestogen component of HRT
42.
Progestogen-only pill (POP)?
No age restriction for the POP and it can be used
safely until a woman no longer requires
contraception.
The POP is not licensed for use as endometrial
protection with oestrogen replacement and should
not be used as the progestogen component of HRT
Case 7
MRS.X ,29YEAR OLD,P1L1,FORGETS TO TAKE
PROGESTERONE ONLY PILL SCHEDULED THAT
MORNING, AS SHE WAS BUSY TAKING HER BABY FOR
THE FIRST PENTAVALENT VACCINATION.
SHE REALISED THE MISSED PILL ON RETURNING HOME
BY LATE NIGHT.
SHE SEEKS YOUR ADVICE
To take 1 pill ASAP.
To use additional contraception for next 48 hours.
46.
POPS
steady levels ofprogestogen are acheived in 4-5 days.
MOA:
1.cervical mucus effect
2.inhibition of ovulation
3.acclerated tubal motility
4.endometrial alteration
optimal cervical mucus effect :begins after 2hours and
lasts for 23hours.
47.
Case 8
30 YRSOLD,MRS.ANTARA,P1L1A1,USING DMPA
INJECTION FOR CONTRACEPTION FOR PAST ONE
YEAR,PLANS FOR EUROPE TOUR WITH FAMILY.
HER CONCERN IS THAT HER TRIP DATE COMES 1 WEEK
PRIOR TO THE SCHEDULED DATE OF DMPA INJECTION.
HELP HER.
GIVE THE USUAL DOSE OF INJECTION
DMPA can be safely given 2 weeks before or upto 1 month
after the scheduled date.
48.
DMPA
Micro crystals ofprogestin
a single 150mg inj can suppress ovulation for 14weeks.
Return of fertility: 70% conceive in 12months
90% conceive in 24months
Does not impair lactation
bone mineral loss with recovery of bone mass after
discontinuation
benefits women with SICKLE CELL DISEASE.
49.
Case 9
33 YEAROLD MRS.CHHAYA,EVENT MANAGER,ON
ORMELOXIFENE SINCE TWO MONTHS BACK,
MISSES THE SECOND PILL SCHEDULED FOR THAT
WEEK BY 2 DAYS.
SHE SEEKS YOUR ADVICE
take the pill ASAP
Maximum serum concentrations are achieved in 3-8
hours of administration
Mean residence time : 128 days.
50.
CENTCHROMAN
Ormeloxifene,nonsteroidal selective estrogenmodulator.
Has weak estrogen agonistic activity in bones and
potent anti estrogenic activity in uterus and breast.
MOA : asynchrony in menstrual cycle between
endometrium and developing embryo resulting in
implantation failure.
dose: 30 mg twice weekly for 1st 3 months followed by
once weekly.
other uses: AUB, mastalgia
51.
Case 10
A 28/fMrs Mirena P1L1 /Immediate
postpartum,wants to delay her next
child birth. Not willing to take any
oral medication/ injections
How would you help her?
52.
CONTRACEPTION IN
LACTATING MOTHER
Barriermethods,spermicides,the copper T380A
good options.
Progestin only OCs,implants and injectable
contraceptives do not effect milk quality/quantity
progestin only pills/ Implants can be started
immediate postpartum
DMPA can begin at 6 weeks.
53.
Case 11
Mrs ssss,28years/P2L2/previous
normal delivery with cuT375, LCB
8months,was on regular follow up has
now come to your OPD with C/O not
able to feel the CuT thread and
amenorrhoea for 1 month.
how do you manage?
54.
do UPT andUSG pelvis.
if UPT -NEG ,USG CuT Insitu--REASSURE
if UPT -neg,USG displaced CuT --usg
guided/hysteroscopic removal
If UPT -POSITIVE,
1.Therapeutic abortion
2.USG guided intra uterine removal of the IUD
3.Continuation of pregnancy with device left in situ
#10 It is appropriate to screen for STIs and place an IUD on the same day. Screening and awaiting results before IUD insertion do not decrease the risk of postinsertion PID but could delay initiation of highly effective contraception and increase the risk of unintended pregnancy.
#11 A retrospective review of 2,138 adolescents and women aged 13–35 years with an IUD showed that younger females (aged 13–19 years) and nulliparous women were not more likely to experience expulsion than older or parous women
A prospective study that compared 12-month pregnancy rates of 69 participants aged 18–35 years from the CHOICE project who had discontinued their IUD with 42 former non-IUD users found no difference in pregnancy rates or time to pregnancy between the groups
#13 etonogestrel implant users,
The CDC recommends consideration of the following two treatment options: 1) NSAIDs for short-term treatment (5–7 days), and 2) hormonal treatment (if medically eligible) with low-dose combined oral contraceptives or estrogen for short-term treatment (10–20 days)
#15 use of DMPA is associated with loss of bone mineral density (BMD), current longitudinal and cross-sectional evidence suggests that recovery of BMD occurs after discontinuation of DMPA. No high-quality data answer the important clinical question of whether DMPA affects fracture risk in adolescents or adults later in life. “black box” warning to DMPA labeling about the potential loss of BMD. The potential health risks associated with the bone effects of DMPA must be balanced against a woman’s likelihood of pregnancy using other methods or no method, and the known negative health and social consequences associated with unintended pregnancy, particularly among adolescents
#18 BMI should be documented for all women prior to CHC prescription. Pelvic examination is not required prior to initiation of CHC. Breast examination, cervical screening, testing for thrombophilia, hyperlipidaemia or diabetes mellitus and liver function tests are not routinely required prior to initiation of CHC.
#19 CP- s 33.9 micrograms ethinylestradiol and 203 micrograms norelgestromin per 24 hours (Evra®). One patch to be applied once weekly for three weeks, followed by a 7 day patch free interval.
CVR: f ethylene vinylacetate (latex-free) and releases 15 micrograms ethinylestradiol and 120 micrograms etonogestrel daily. One ring should be inserted vaginally for 3 weeks of use per cycle. Rings must be kept refrigerated prior to dispensing to the client. Thereafter, they can be stored at room temperature and used within 4 months
#20 combined hormonal contraception (CHC) is as safe and at least as effective for contraception if it is taken as an extended or continuous regimen
#32 single dose of 1.5 mg, or alternatively in 2 doses of 0.75 mg each, 12 hrs apart).
UPA had a pregnancy rate of 1.2%. LNG had a pregnancy rate of 1.2% to 2.1% . Yuzpe regimen (one dose of 100 μg of ethinyl estradiol & 0.50 mg of LNG, followed by a second dose of same 12 hrs later).
#36 Women aged over 40 years have a distinct set of needs regarding contraception. Perimenopausal symptoms (e.g. vasomotor symptoms, mood changes, irregular and/or heavy bleeding) combined with increased background risks of certain health conditions (e.g. cardiovascular disease, obesity, breast cancer, most gynaecological cancers) mean that the benefits and risks of contraception for this population are different from those relevant to younger women.
#37 The risk of venous thromboembolism (VTE) increases sharply over the age of 40 years, which means that consideration of other risk factors for VTE is essential when considering CHC in this age group. Weight is an important risk factor; body mass index should be reviewed on a regular basis.1 The risk of VTE is highest on initiation of CHC and this increased risk recurs if CHC is stopped and restarted.1 The guideline therefore advises against repeated episodes of stopping/starting CHC, for example, to measure follicle stimulating hormone (FSH) levels. Pills containing higher doses of oestrogen are linked to greater risk of VTE, stroke, and cardiovascular disease.1 When prescribing COC for women over 40, first choice should be a preparation with ≤30 mcg ethinylestradiol. This should be combined with either levonorgestrel or norethisterone as this combination confers the lowest VTE risk.
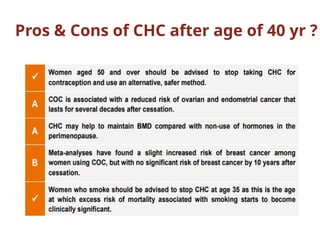
Women aged over 35 who smoke and all women aged over 50 (regardless of smoking status) should be advised to stop CHC as risks outweigh benefits
#39 If only being used for HMB and/or menstrual pain (not contraception or endometrial protection), can remain in situ for as long as it controls symptoms, regardless of age at insertion.
#41 Depot medroxyprogesterone acetate (DMPA) is associated with a reduction in bone mineral density (BMD) in women of all ages.1 Reassuringly, studies looking at women over 40 who use DMPA have shown that although users experience an initial loss in BMD with use, this is not repeated or worsened by menopause.1 Women over 40 with additional risk factors for osteoporosis are advised to consider alternative methods.