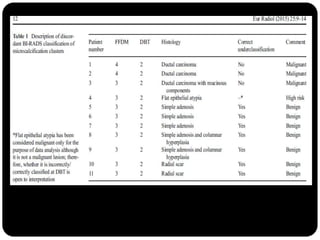
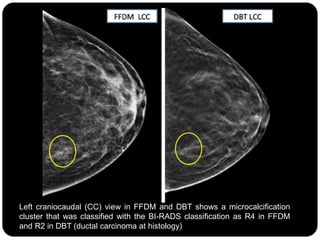
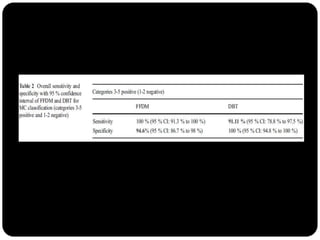
This study compared the characterization of microcalcification clusters using 2D digital mammography (FFDM) and digital breast tomosynthesis (DBT) in 107 cases. There were 11 discordant results where DBT classified clusters lower than FFDM. DBT incorrectly underclassified 3 clusters as benign that were malignant. However, DBT correctly classified 8 clusters as benign that FFDM misclassified as suspicious. While diagnostic performance between the two modalities was similar, the authors conclude DBT has the potential to underestimate a small portion of malignant lesions, so 2D plus 3D imaging is recommended for breast screening to avoid missing microcalcification clusters.