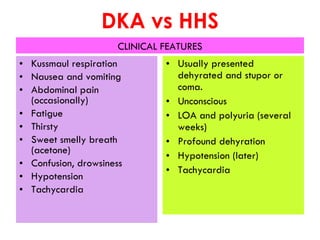
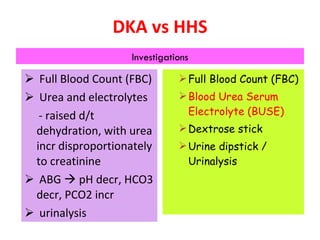
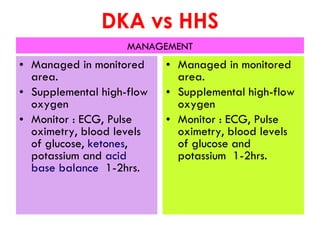
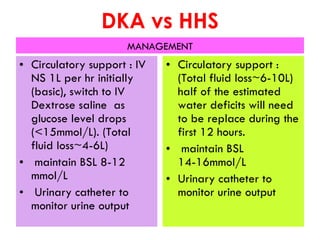
The document presents two clinical cases distinguishing between diabetic ketoacidosis (DKA) and hyperglycemic hyperosmolar state (HHS). It outlines the symptoms, diagnostic criteria, and management of each condition, highlighting the differences in patient presentations and mortality rates. The first case is indicative of DKA in a 60-year-old man, while the second case suggests HHS in a 25-year-old woman.












































































![Hyperosmolar Non Ketotic Dm [Autosaved]](https://cdn.slidesharecdn.com/ss_thumbnails/hyperosmolarnon-ketoticdmautosaved-091102093711-phpapp02-thumbnail.jpg?width=640&height=640&fit=bounds)




























