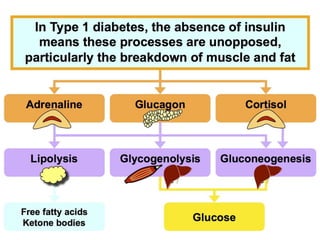
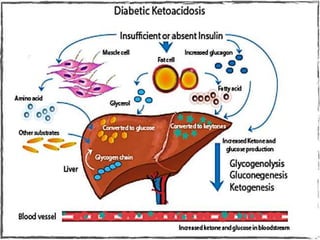
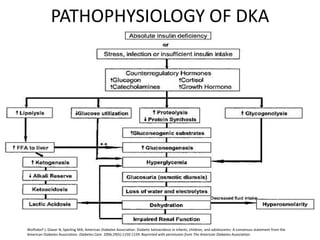
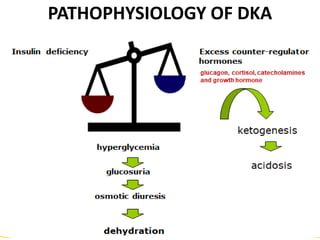
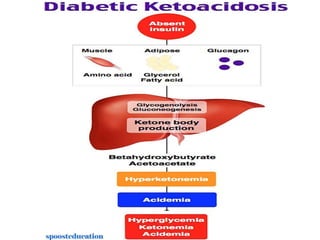
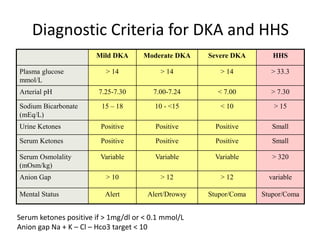
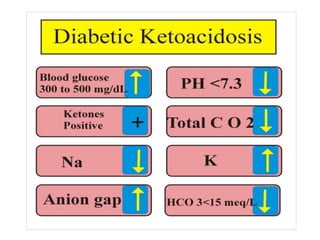
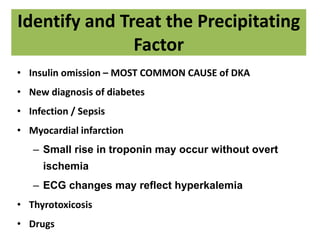
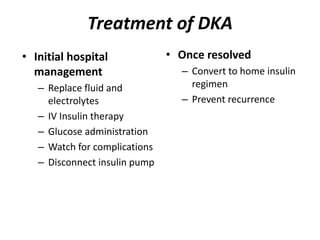
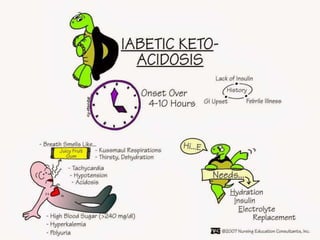
Diabetes is a condition where the body does not properly process glucose due to lack of insulin or insulin resistance. Diabetic ketoacidosis (DKA) occurs when a lack of insulin causes the body to break down fat and produce ketones, leading to hyperglycemia, ketosis and acidosis. DKA treatment involves rehydration, insulin therapy to lower blood glucose and ketone levels, electrolyte replacement, and identifying/treating the precipitating cause. Complications can include infection, shock, cerebral edema and death if not properly managed. Prevention relies on education about sick day management to avoid DKA during illness.