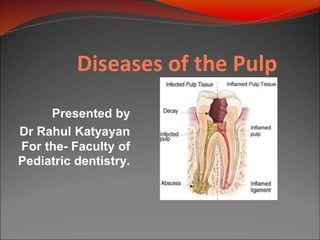
Diseases of pulp
•Download as PPTX, PDF•
5 likes•360 views

This document provides an overview of diseases of the pulp. It discusses pulpitis, which is inflammation of the pulp that can be reversible or irreversible depending on the severity. Reversible pulpitis involves mild inflammation that can return to normal, while irreversible pulpitis is persistent and may lead to necrosis without treatment. Other topics covered include causes of pulp inflammation, classifications of pulpitis, features of acute and chronic pulpitis, necrosis, and management approaches for different pulp conditions. The document aims to inform pediatric dentists about diseases that can affect the pulp.

More Related Content
What's hot
What's hot (20)
Similar to Diseases of pulp
Similar to Diseases of pulp (20)
Recently uploaded
Recently uploaded (20)
Diseases of pulp
- 1. Diseases of the Pulp Presented by Dr Rahul Katyayan For the- Faculty of Pediatric dentistry.
- 2. CONTENTS ⚫ INTRODUCTION ⚫ PULPITIS ⚫ SEQUELAE ⚫ CAUSES ⚫ CLASSIFICATION ⚫ REVERSIBLE PULPITIS ⚫ FOCAL REVERSIBLE PULPITIS ⚫ IRREVERSIBLE PULPITIS ⚫ ACUTE PULPITIS ⚫ CHRONIC PULPITIS ⚫ NECROSIS ⚫ REFERENCES
- 3. ⮚ formative organ of tooth ⮚ builds primary dentin during development of tooth ⮚ secondary dentin after tooth eruption ⮚ reparative dentin in response to stimulation as long as odontoblast remain vital Pulp
- 4. ⮚ most common cause of dental pain ⮚ loss of teeth in younger persons ⮚ usual cause is caries penetrating the dentin Pulpitis
- 5. Pulpitis UNTREATED Death of pulp Spread of Infection through apical foramina into periapical tissues Causes Periapical Periodontitis
- 6. ⮚ (1)Physical Cause a)Mechanical b)Thermal ⮚ (2) Chemical Cause ⮚ (3) Bacterial Cause Causes of Pulpal Inflammation
- 7. ⮚ (a) Mechanical Cause A. trauma a) accident (contact sports) b) iatrogenic damage due to dental procedure (during cavity or crown preparation) B. Pathologic wear ( atrrition, abrasion) C. Cracked tooth syndrome D. Barometric changes Causes of Pulpal Inflammation
- 8. ⮚ (b) Thermal Cause ✔ uninsulated metallic restoration ✔ during cavity preparation ✔ polishing Causes of Pulpal Inflammation
- 9. ⮚ (2) Chemical Cause ✔ arise from erosion ✔ or inappropriate use of acidic dental material Causes of Pulpal Inflammation
- 10. ⮚ (3) Bacterial Cause ✔ can damage pulp through toxins secreted by bacteria from caries ✔Microbial colonization in the pulp by blood borne microorganisms (anachoresis). Causes of Pulpal Inflammation
- 11. ⮚ (1) Based on Severity of Inflammation ⮚ (2) According to Involvement Classification
- 12. ⮚ (1) Reversible Pulpitis ⮚ (2) Irreversible Pulpitis ⮚ (3) Pulp Degeneration ⮚ (4) Pulp Necrosis (1) Based on Severity of Inflammation
- 13. ⮚ (1) Reversible Pulpitis ✔ Symptomatic (acute) ✔ Aysptomatic (chronic) ⮚ (2) Irreversible Pulpitis ✔ Acute • Abnormally responsive to cold • Abnormally responsive to heat (1) Based on Severity of Inflammation
- 14. ⮚ (2) Irreversible Pulpitis ✔ Chronic • Asymptomatic with pulp exposure • Hyperplastic • Internal resorption (1) Based on Severity of Inflammation
- 15. ⮚ (3) Pulp Degeneration ✔ Calcific ⮚ (4) Pulp Necrosis (1) Based on Severity of Inflammation
- 16. ⮚ (1) According to extent of inflammation ⮚ (2) According to Severity ⮚ (3) According to presence or absence of direct communication between dental pulp + oral environment (2) According to Involvement
- 17. ⮚ (1) According to extent of inflammation ✔ Focal or Subtotal or Partial Pulpitis ✔ Total or Generalized Pulpitis (2) According to Involvement
- 18. ⮚ (2) According to Severity ✔ Acute ✔ Chronic (2) According to Involvement
- 19. ⮚ (3) According to presence or absence of direct communication between dental pulp + oral environment ✔ Pulpitis Aperts (open pulpitis) ✔ Pulpitis Clausa (closed pulpitis) (2) According to Involvement
- 20. ⮚ mild to moderate inflammatory condition of pulp ✔ caused by noxious stimuli ✔ pulp is capable of returning to un-inflammed state following removal of stimuli Reversible Pulpitis
- 21. ⮚ Causes ✔ agent capable of injuring pulp like: • trauma • disturbed occlusal relationship • thermal shock Reversible Pulpitis
- 22. ⮚ Clinical Features ✔ sharp pain lasting for a moment ✔ often brought on by cold than hot food or beverages and by cold air Reversible Pulpitis
- 23. ⮚ Clinical Features ✔ does not continue when the cause has been removed ✔ tooth responds to electric pulp testing at lower current Reversible Pulpitis
- 24. ⮚ Management ✔ prevention ✔ periodic care ✔ early insertion of filling if a cavity has developed ✔ removal of noxious stimuli Reversible Pulpitis
- 25. ⮚earliest form ⮚ also known as pulp hyperemia ⮚ excessive accumulation of blood within pulp tissue ⮚ leads to vascular congestion Focal Reversible Pulpitis
- 26. ⮚ Clinical Features ✔ sensitive to thermal changes ✔ particularly to cold ✔ application of ice or cold fluids to tooth result in pain Focal Reversible Pulpitis
- 27. ⮚ Clinical Features ✔ disappears upon removal of thermal irritant or restoration . ✔ responds to electrical test stimulant at lower level of current Focal Reversible Pulpitis
- 28. ⮚ Clinical Features ✔ indicates lower pain threshold than that of adjacent normal teeth Focal Reversible Pulpitis
- 29. ⮚ Clinical Features ✔ teeth show: • deep carious lesion • large metallic restoration • restoration with defective margins Focal Reversible Pulpitis
- 30. ⮚ Management ✔ removal of irritants before the pulp is severely damaged Focal Reversible Pulpitis
- 31. ⮚ persistent inflammatory condition of pulp ⮚ may be symptomatic or asymptomatic ⮚ caused by noxious stimulus Irreversible Pulpitis
- 32. ⮚ Causes ✔ bacteria involvement of pulp through caries ✔ chemical ✔ thermal ✔ mechanical injury Irreversible Pulpitis
- 33. ⮚ Clinical Features Early Stage ✔ paroxysm of pain caused by: • sudden temperature changes like cold, sweet, acid foodstuffs Irreversible Pulpitis
- 34. ⮚ Clinical Features Early Stage ✔ pain often continues when cause has been removed ✔ may come and go spontaneously Irreversible Pulpitis
- 35. ⮚ Clinical Features Early Stage ✔ pain • sharp • piercing • shooting • generally severe Irreversible Pulpitis
- 36. ⮚ Clinical Features Early Stage ✔ pain • bending over exacerbates pain which • lying down is due to change in • change of position intrapulpal pressure Irreversible Pulpitis
- 37. ⮚ Clinical Features Late Stage ✔ pain • more severe as if tooth is under • throbbing constant pressure Irreversible Pulpitis
- 38. ⮚ Clinical Features Late Stage ✔ pain • patient is often awake at night due to pain • increased by heat and sometimes relieved by cold, although continued application of cold may intensify pain Irreversible Pulpitis
- 39. ⮚ Management ✔ complete removal of pulp or pulpectomy ✔ if the time is a factor, pulpotomy should be done as an emergency procedure ✔ Surgical removal should be considered if the tooth is not restorable. Irreversible Pulpitis
- 40. Clinical Difference Reversible Pulpitis Irreversible Pulpitis ⮚ pain generally lasts for few seconds ⮚ the pain produced by thermal stimulus disappears as soon as the stimulus is removed Pain may last several minutes or later ⮚ pain lingers even after the stimulus is removed ⮚ pain may come without any apparent stimulus
- 41. ⮚ extensive acute inflammation of pulp ⮚ frequent sequel of focal reversible pulpitis Acute Pulpitis
- 42. ⮚ Causes ✔ tooth with large carious lesion ✔ defective restoration where there has been recurrent caries ✔ pulp exposure due to faulty cavity preparation Acute Pulpitis
- 43. ⮚ Clinical Features ✔ severe pain is elicited by thermal changes ✔ pain persists even after thermal stimulus disappears or been removed Acute Pulpitis
- 44. ⮚ Clinical Features ✔ may be continuous ✔ intensity may be increased when patient lies down ✔ application of heat may cause acute exacerbation of pain Acute Pulpitis
- 45. ⮚ Clinical Features ✔ tooth reacts to electric pulp vitality tester at a lower level of current than adjacent normal teeth Acute Pulpitis
- 46. ⮚ Clinical Features ✔ pressure increases because of lack of escape of inflammatory exudate ✔ rapid spread of inflammation through pulp with pain + necrosis Acute Pulpitis
- 47. ⮚ Management ✔ early stages of acute pulpitis pulpotomy (removal of coronal pulp) ✔ placing material that favors calcification such as: • calcium hydroxide over entrance of root canals Acute Pulpitis
- 48. ⮚ Management ✔ root canal filling with inert material like gutta percha should be done Acute Pulpitis
- 49. ⮚ may develop with or without episodes of acute pulpitis ⮚ many pulps under large carious cavities die painlessly ⮚ 1st indication is then development of periapical periodontitis, either with pain or seen by chance in radiograph Chronic Pulpitis
- 50. ⮚ Clinical Features ✔ dull aching type ✔ more often intermittent than continuous Chronic Pulpitis
- 51. ⮚ Management ✔ root canal therapy ✔ followed by crown restoration Chronic Pulpitis
- 52. ⮚ also called as pulp polyp or pulpitis aperta ⮚ essentially an excessive exuberant proliferation of chronically inflammed dental pulp tissue Chronic Hyperplastic Pulpitis
- 53. ⮚ pulpal inflammation due to an extensive carious exposure of a young pulp ⮚ development of granulation tissue ⮚ covered at times by epithelium ⮚ resulting from long standing low grade infection Chronic Hyperplastic Pulpitis
- 54. ⮚ Causes ✔ slow progressive exposure of pulp ✔ bacterial infection Chronic Hyperplastic Pulpitis
- 55. ⮚ Clinical Features ✔ most commonly involved are deciduous molars + 1st permanent molar • excellent blood supply • large root opening Chronic Hyperplastic Pulpitis
- 56. ⮚ Clinical Features ✔ asymptomatic ✔ seen only in teeth of children + young adults Chronic Hyperplastic Pulpitis
- 57. ⮚ Clinical Features ✔ polypoid tissue appears • fleshy • reddish pulpal mass filling most of pulp chamber or cavity • or even extend beyond confines of tooth Chronic Hyperplastic Pulpitis
- 58. ⮚ Clinical Features ✔ polypoid tissue appears • sometimes, if mass is large enough • interferes with closure of mouth Chronic Hyperplastic Pulpitis
- 59. ⮚ Clinical Features ✔ polypoid tissue appears • may cause discomfort during mastication • due to pressure of food bolus Chronic Hyperplastic Pulpitis
- 60. ⮚ Clinical Features ✔ polypoid tissue appears • tissue easily bleeds because of rich network of blood vessels • tooth may respond or not at all to thermal test Chronic Hyperplastic Pulpitis
- 61. ⮚ Management ✔ elimination of polypoid tissue ✔ followed by extirpation of pulp ✔ hyperplastic tissue bleeeding can be controlled by pressure ✔ pulpectomy or extraction of tooth can also be done if the tooth is not restorable. Chronic Hyperplastic Pulpitis
- 62. ⮚ death of pulp ⮚ may be partial or total depending on whether part or the entire pulp is involved Necrosis
- 63. ⮚ Causes ✔ sequeala of inflammation ✔ can also occur following trauma • pulp is destroyed before an inflammatory reaction Necrosis
- 64. ⮚ Types ✔ (1) Coagulation Necrosis ✔ (2) Liquefaction Necrosis Necrosis
- 65. ⮚ Types ✔ (1) Coagulation Necrosis • soluble portion of tissue is precipitated or converted into a solid material Necrosis
- 66. ⮚ Types ✔ (1) Coagulation Necrosis • tissue is converted into tissue mass consisting chiefly of coagulated ▪ proteins ▪ fats ▪ water Necrosis
- 67. ⮚ Types ✔ (2) Liquefaction Necrosis • results when proteolytic enzymes convert the tissue into softened mass liquid or amorphous debris Necrosis
- 68. ⮚ Clinical Features ✔ no painful symptoms ✔ discoloration of tooth • 1st indication that the pulp is dead Necrosis
- 69. ⮚ Clinical Features ✔ history of pain lasting from a few minutes to a few hours followed by complete + sudden cessation of pain Necrosis
- 70. ⮚ Management ✔ preparation + obturation of root canals Necrosis
- 71. References: ❖ Books ⮚ Grossman’s endodontic practice twelfth edition ⮚Textbook of oral pathology shafers ⮚Cawson, R.A: Cawson’s Essentials of Oral Pathology and Oral Medicine, 8th Edition.(page 60) ⮚ Ghom, Ali & Mhaske, Shubhangi: Textbook of Oral Pathology. (pages 420-425)
- 72. References: ⮚Adrian,J.C.,et al.:J. Am. Dent. Assoc.,83:113, 1971. ⮚Allard, U., et al.:Oral Surg.,48:454, 1979. ⮚Austin, L.T.:J. Am. Dent. Assoc.,17:1930, 1930. ⮚Baume, L.: SSO Schweiz. Monatsschr. Zahnheilkd.,77:1082, 1965.
- 73. References: ⮚Baume, L.: Transactions of the Fourth International Conference on Endodontics. Philadelphia: University of Pennsylvania press, 1968, p. 66 . ⚫Baume, L.J.: Monogr. Oral Sci.,8:1- 220, 1980.
- 74. THANK YOU