Downloaded 234 times




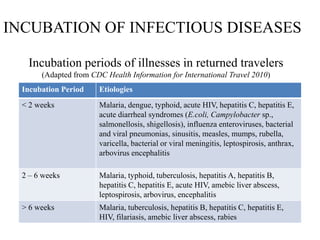
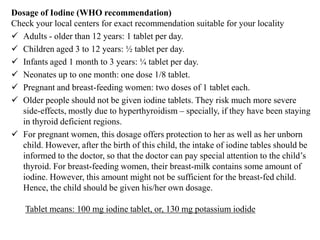



This document provides an overview of disaster management. It begins with definitions of disasters and emergency management. It describes the different types of natural and man-made disasters. It outlines the disaster management cycle, including the disaster phase, response phase, recovery phase, risk reduction phase, and preparedness phase. It discusses victims and survivors of disasters and the concept of a "second disaster". It also covers topics like disaster syndromes, examples of past disasters, patterns of injury and mortality, displacement of victims, impacts on health, and approaches for specific disasters like floods, earthquakes, and nuclear incidents.












































































