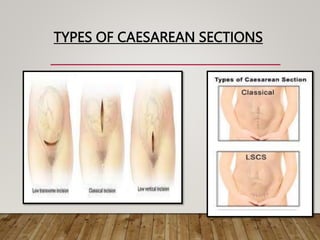
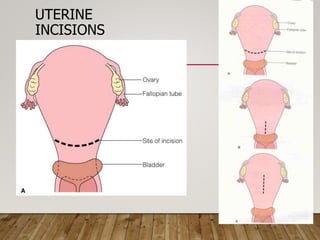
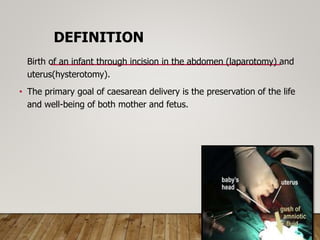
Caesarean section, also known as a C-section, is the surgical delivery of a baby through incisions in the abdomen and uterus. It is performed when vaginal delivery would put the mother or baby's life at risk or in other complicated pregnancies. There are two main types of uterine incisions used - the lower uterine segment incision and the classical or upper segment incision. While C-sections can save lives, they also carry risks for both mother and baby, such as infection, bleeding, injury, and complications with future pregnancies. Post-operative care involves monitoring for issues like fever, heavy bleeding or wound separation.

![Relative indications:
• Cephalo-pelvic disproportion
• Previous caesarean delivery
• Non reassuring FHR (fetal distress)
• Dystocia [due to (three Ps) relatively large fetus
(passenger), small pelvis (passage) / or inefficient
uterine contractions (power)]
• Ante partum hemorrhage (APH)
• Malpresentations
• Failed surgical induction of labor
• Failure to progress in labor.](https://image.slidesharecdn.com/cesareansection-230823091446-d5a22ce9/85/CESAREAN-SECTION-pptx-6-320.jpg)